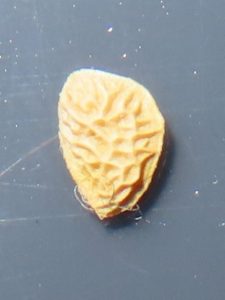
Wearing the T shirt that I had printed more than 2 years ago; when I knew that I had solved this medical mystery!
Cure For Morgellons Disease
Introduction
My name is David Payne, I am not medically trained, merely the Morgellons Disease patient who refused to waste his life waiting for ‘medical science’.
This I have written as the layman that I am for the benefit of other laymen, however, I have learned the hard way that laymen won’t listen until doctors have, which task has proven to be an even greater challenge!
The official figure I found for MD is claimed at around 14,000 families, however, doctors are so incapable of diagnosing this complaint the true figure could actually be in the millions?
Subsequently, the Charles E. Holman Morgellons Disease Foundation informed me that “the CDC now admits that at least 500,000 are infected annually in the U.S. alone!
Those are only the ones who get diagnosed and reported. The current tests are known to miss over half the cases.”
Every Morgellons Disease patient has a horror story about the incompetence of medical science; consequently, it’s not possible for this to be written without that negativity influencing the positive content. Nevertheless, I have no doubt whatsoever that it’s way past time for these elephants in the room to be exposed!
I decided that ‘scathing’ is an essential element, which may only become obvious to those who can understand. The enormity of this document is too important to be ignored and if I don’t take this opportunity to expose a few of these elephants in the room, maybe no one else ever will; in for a penny in for a pound. There are doctors who need reminding that they are doctors and medical science needs reminding that their job is healthcare not wealth-care. This dissertation would remain highly controversial even without the scathing, however, not being part or politic of the ‘system’, I have nothing whatsoever to gain from polite ignorance; consequently, I have nothing to be lost. This document was born as a collection of; the good, the bad and the ugly notable happenings that I have recorded along the way which over time has metamorphosed into this.
Following 7 years of incorrect diagnosis from a long list of doctors and dermatologists including; folliculitis, impetigo, scabies, dermatitis, eczema and delusional parasitosis with recommendation for Cognitive Behaviour Therapy and also Paranoid Personality Disorder, which I have ‘avoided’ with a private diagnosis by a professor to be ‘Unexplained Dermopathy’, who prescribed doxycycline and instructed me to continue using Trimovate cream, then referred me back to the NHS. Following which; his diagnosis was dismissed and ignored by both my GP and the local hospital, from where I was incorrectly discharged twice and required the assistance of my MP to even be seen, whereupon my 6-month review was incrementally extended to 26-months. During which time included; battling with dermatologists for the antibiotics required, followed by my GP refusing to issue the Trimovate that he had prescribed, followed by several further battles with a senior dermatologist and my GP to prevent the antibiotics prescribed by the professor from being terminated by ‘doctors’ who wouldn’t even examine me because they have incorrectly ‘labelled’ me with their imaginary mental health issues!
During these 26 months of being avoided by the people who are paid to be my care providers; I unravelled the Morgellons Disease mystery, exposed its biology, discovered and formulated a cure and successfully administered this on myself.
I have beaten MD not because of medical science, yet mostly despite it!
The greatest handicap to this recovery was my GP and the local hospital with whom I have tried to share my findings. Initially, I thought myself ‘unfortunate’ to have become saddled and bracketed with/by an incompetent ignorant bigot GP and a common or garden ignorant bigot senior dermatologist; however, I have since learned from online reports by others that this appears pretty much standard malpractice for MD sufferers. Nevertheless, having only incorrect boxes to tick for Morgellons Disease has resulted with many doctors complying with this misguided State sponsored mass psychogenic disorder which trains them to not step outside of the boxes and which disallows their brains to believe their eyes and ears. You couldn’t make this ridicule up, quite literally; professional insanity!
Following peer approval of the facts presented in this dissertation, I will send a copy to the General Medical Council and press for an official enquiry into this heinous malpractice of a ‘doctor’ who clearly doesn’t understand the difference between “Hippocratic” and “Hypocrite”!
For deliberately hindering my remission, he should be struck off the Doctors Register and for trying to prevent this cure from being administered and proven to benefit billions; imprisoned!
Maybe this evidence based document should become compulsory remedial bedtime reading for him; after he has cleaned the prison toilets and shared a shower with inmates?
Following more than 400 years of failure by medical science with $millions spaffed on ‘research’ for men in white coats to aimlessly peer into microscopes, notwithstanding, the many $millions more that patients have paid to doctors who can’t cure this and many $millions more spent on medications that don’t work; collectively, these factors indicated that an alternative approach was required; consequently, I focused my divergent mind on areas that were of least interest to previous research. Primarily, “how MD feels”, describing how this ailment feels to a doctor can result with being locked up in a Psychiatric Hospital and incorrectly subjected to CBT, so it’s hardly surprising that nothing has been learned by medical science here!
I have experienced so much ignorance and bigotry from ‘medical science’; I’m amazed how anything has been learned at all?
Subsequently, I have taken a very deep dive into this great unknown where Angel’s have feared to tread and my analysis of these previously ignored feelings was the route to a solution. Physically, I focussed on the ‘keratin’, which rarely gets a mention.
Stating what should be obvious; this information is ‘Hot off the Press’.
I am literally writing this dissertation with one hand, whilst nursing myself better with the other. My ambition is; to have this writing completed to coincide with full remission, the date of which I await to learn. There are so many things that require explaining without words that adequately describe them; there will always remain addendums. Nevertheless, also my best means of recording this apparently not so abstract information for posterity.
A Positive Mental Attitude is requisite for this cure and here practicing what I preach.
I AM DOING THIS BECAUSE I CAN!
I have not obsessed over this with a microscope, ‘merely’ experimented with alternative products and interpreted what my body was telling me, whilst also gleaning further details from reading many thousands of pleas for help by desperate others ignored by doctors; to which I applied my analytical skills.
No white coats were harmed by my research.
There was no need; the component parts of this infection/organism can be seen with the naked eye, each has a different ‘character’ and each with an alternative Achilles heel.
Along this journey, I learned the hard way that ‘feeling-better’ is not ‘getting-better’ and that getting better is not feeling better at all and ultimately, gaining understanding of how to manage these ‘getting-better’ feelings.
This is not merely a ‘pop the pills until it goes away’ remedy, or a David’s Magic Potion, but a somewhat bizarre lifestyle program that incorporates readily available mineral and herbal products which assist antibiotics with the cure. The least abstract and most comprehensible explanation that I can provide is to describe this as like a combination lock, however, instead of having just 4 digits, there are about a dozen that must be lined up correctly for keratinocytes remission to begin, which results with around 4-6 hours of exfoliation before MD automatically re-locks, or you are tired and go to bed. You literally have to ‘fool’ MD out of your body whilst not losing your marbles. Learning how to achieve this required IMMENCE power of will; nevertheless, my strength to beat this explained as best I can, makes this previously impossible task achievable by others less able.

Like tumblers in a combination lock
There is no need whatsoever to go at this like a bull in a china shop, remission progresses like paying off a debt. You line up the tumblers in MD’s combination lock and then exfoliate for around 4 or 5 hours per day at a ‘speed’ that is ‘comfortable’ for you. This you do as if it was the job of a nurse. You can take breaks for holidays and pick up where you left off when you get home. Every evening/night spent exfoliating, is one step closer to the end of this very long tunnel. This you continue and repeat until MD has gone and then after you have forgiven me, maybe you might treat me to a beer?
MD will fight back every inch of the way as if it was strategy of a sentient being, with ways and means that you won’t see coming and/or ways that you couldn’t imagine and by obscure means that you may deny yourself for your own detriment that is advantageous to it. To beat this you need to declare war and will be the greatest challenge you have ever faced that nobody other than fellow MD convalescents will be able to understand.
MD directly influences you to eat lipids and sugars, be lazy and fat, to not drink enough and dissuades you from moisturising your skin; which results with MD getting more of its favoured sustenance and which also creates more prime real estate for MD to colonise.
Underneath hair anywhere on the body is the ‘Beverly Hills’ for MD, consequently, it doesn’t like short haircuts and loves a Growler and/or a beard.
Denial of this/these, is evidence that MD has you under its control and you will NEVER beat it
To suggest addressing any of these matters to an MD ‘addict’ is highly likely to result with an illogical and/or emotional response!
Should you require a parallel to get your head around this, the simplest description that I can provide would be to suggest that you watch a film/movie called ‘Venom’. Morgellons could be described as his invisible cousin.

I make no secret that remission from this remarkably tenacious ailment is a greater challenge than the complaint, this is often unpleasant, occasionally painful and challenging in ‘special’ ways, sufficient to qualify as a ‘Rite Of Passage’; however, it would be wishful thinking to expect anything other from MD. Neither is this a ‘quick fix’. Remission is slow; which is a blessing and not a curse, because the faster the remission, especially during the early stages, the greater the discomfort can be. When you do something that hurts MD, it will punish you by hurting you back to try and stop you. The more that it hurts, the more MD is losing. The art of remission is to manage these discomforts to remain within your tolerance. You MUST be extremely determined to succeed.
It took me around 2 years of intensive self nursing to beat this, with the first year spent thinking that it would never come out of my skin and with the second spent thinking that it would never stop coming out of my skin. Nevertheless, during this time I continued to identify ways and means of improving this remedy, it’s remarkable how much difference that somewhat unobvious details can and do make and I am confident that diligent application of my final best found practice could result with beating this ailment in far less time than it took me and with far less discomfort. Armed with understanding of what the bizarre sensations are that are happening in the skin removes their mystery and leaves these Gremlins nowhere to hide.

Approaching 4 million of this volume!
For something that can be clearly seen by anyone who has not been brainwashed by the ‘system’, remarkably, this can’t be seen by around 99.99% of doctors, dermatologists, pathologists or scientists and consequently, officially doesn’t exist; there is an amazing/unbelievable/unimaginable amount of it. The volume of keratin (ocytes), ‘sores’ and last but definitely not least the fibres and micro fibres that is/are in the skin and which all must be exfoliated, is/are way beyond belief, it is not possible to even imagine their extensiveness which could maybe best be described as a singularity of keratinocytes that encapsulates each & every microfibre, fibre, and sore, the ‘decompressed’ volume of which will exceed any and every preconception you could possibly have, every single day until it has gone!
To provide a frame of concept for this volume, I estimate that a deposit averaging the size of a marrowfat pea was incrementally exfoliated from every follicle and there are almost 4 million of those! Describing alternatively; after the massive amount of immeasurable magically disappearing keratinocytes had cleared; an average of around 100ml of quantifiable debris was exfoliated every day for 14 months, which equates to around 42 litres.
Presently, the only helpful thing that any doctor is capable to do, is to issue a repeat prescription for the antibiotics, from there on in; you are your own physician. Pay close attention to what may appear to be the unlikeliest of details in the program or you may achieve no positive results at all, or worse. Administration of this cure is an obscure art that will vary dependent on each person’s individual constitution.
It’s no secret that MD is difficult to describe; this is a remarkably slippery subject in far more mysterious ways than one and translating these abstracts into realities conspired for this dissertation to be a most challenging prose. For which, I haven’t endeavoured to utilise a medical dictionary which should make it easier for MD sufferers to understand, nevertheless, I strongly suspect those would not contain words that are required? If they did, maybe doctors wouldn’t be incorrectly translating patient’s attempts of description as a mental health issue!
No doubt medical science will complain that I haven’t researched this properly, like how they have been unsuccessfully researching properly for too long. There’s more than one way to skin a cat! Alternatively, with parallel logic and without influence from failed research, I have succeeded by using what is now a proven research technique from interpreting what my skin was telling me; which lead to exposing MD’s biology and identifying a cure?
“This information is worthless without peer reviews!”
Are there any peers awake in the audience?
Many have stated online that they would gladly give $10k to consult with a doctor who could cure them of this ailment. However, until the day comes when doctors are required to learn this new field of medicine, folk will have to get by with me curing them for free, however, if they insist, I wouldn’t be offended.
Has anyone seen my cat?
Welcome to the Darwinian rabbit hole where Doctor Dolittle found Schrödinger’s cat”!
I believe that in ‘Rosetta Stone’ manner, my work reveals solutions for more medical mysteries than merely Morgellons which could benefit more than half of the people on our planet.
Freely given; please make of this what you wish.
……………
Unexplained Dermopathy Explained
Morgellons Disease is not a mental health problem that medical science yet understands. Psychiatry has been misled by dermatology; parasitosis is real!
To respond with denial for these strange, painful and (previously) unexplainable happenings, whilst incorrectly accusing patients of mental health problems they don’t have; is psychological torture, which inexorably leads to less ability for rational thought and which is a consequent mental health problem that ignorant bigot doctors are guilty of causation. Resulting with an additional mental health problem because psychiatry hasn’t paused to think! Nevertheless, after psychiatrists have had this check-up from their neck up, maybe they could do what they are supposedly paid for and provide some healthcare by helping MD patients to overcome the Psychodermatological influence of this infection and recover?
It appears that I am the first ever person to have been strong enough to resist this heinous incompetence and then to return and prove these errors beyond any doubt.
Let us hope that my endeavours to persevere are not wasted?
Meanwhile, incompetent bigot doctors have continued to follow me around dishing out accusations of imaginary mental health problems like Green Shield stamps!
From the day that I contracted this ailment when I almost died from hydrogen sulphide gas poisoning, I have now endured incompetent doctor’s imaginary accusations of psychosis, delusional parasitosis and paranoid personality disorder, because they refused and/or were not allowed to believe me! I have literally been persecuted with life endangering levels of stress. I suspect that ignorant bigots deliberately use this as a weapon of deterrence to inhibit patients from returning to challenge them with a subject they know nothing about?
However, despite these heinous activities, I remain positive and hand to them on a plate an opportunity to do something useful that none of them have been bright enough to work out!
I believe that MD has psychological influence at a deeper level to become Master of its own destiny. Such concept could be thought difficult to prove; ironically however, if/now identified, this Gremlin has nowhere to hide!
It looks like my degree in psychology might come in handy again?
I have discovered an open minded Darwinian Psychodermatological solution for this age old medical mystery, which connects dots between alternative fields of medical science and has drawn into light abstract others.
Morgellons Disease is an Autoimmune Disorder that may be described as an ‘Obligate Parasitic Extremophile Acidophilic Photoreactive Aerotolerant/Moderate/Strict/Obligate Anaerobic Organism’ that becomes biologically integrated into the skin and which I believe to be an Archaea not yet identified by medical science. (OPEAPAMSOAA) This organism hijacks the immune system for its own benefit and subsequently, becomes encapsulated within an ever strengthening shield of keratinocytes. By design of evolution, this immune system frontline response has several properties/functions/abilities including a tenacious bond which locks this into the skin. Not only is MD resistant to this defence; but utilises this for its own advantage with every pocket/follicle/sweat-gland of infection being independent from all others and supportive to neighbouring infection. The consequent relentlessly developing and concentrating shield of keratinocytes being produced by the body hides this complaint from diagnosis and defends it from both oral and topical remedies.
MD was airborne when I contracted this ailment 5th November 2014, late in the evening of a very rainy day, rainwater backed up in a faulty sewer which caused hydrogen sulphide gas to rise up an ‘illegal’ vent/stench pipe and into my home, fortunately, I managed, but only just, to get outside before ‘knock down’ and projectile vomiting. This event was a very close encounter with death. Nevertheless, whilst feeling this heavy gas flowing across my face I also experienced a sensation similar to being swarmed by miniscule Scottish midges! At that time I didn’t realise what caused this, however, I now understand this to have been the keratinocytes leaping into action and encapsulating MD. (The concentration of H2S was strong enough for this to be seen floating on the lavatory water looking like mercury.)
Subsequently; my ENT specialist found that this gas had burned off all of the nasal polyps that had previously been in my sinuses. Nevertheless, he was aghast at me for suggesting; maybe the same positive result could be achieved in a controlled manner to benefit others?
Ironically, the stronger the infection, the more covert this organism is enabled to be and consequently, the more difficult for doctors of dermopathy to explain. The stronger the H2S MD matures in, the stronger the acidophiles become, consequently, the stronger the keratin becomes, the stronger the airtight plugs become, the more covert the infection.
Morgellons Disease microfibres populate into every single follicle which ultimately reveal in several different forms, with these ‘core’ element microfibres being the most difficult to identify. The sores are an alternative biological development with the purpose of producing and radiating this acidophiles ‘control’ element over the keratinocytes, what was relevant for me however, MD in this form is susceptible to long term antibiotics.

Fibres producing endospore
These ‘strange’ sores on/in which the largest ‘hairs’ develop were most prolific on the scalp and shoulders which develop to be the largest and deepest over and penetrating into the largest muscles; namely biceps, thighs and calves. It is these revealed and unrevealed sores that are the ‘hive’ source of influence over keratinocytes and which assists proliferation elsewhere, where fibres develop inside little kidney bean shaped endospores before then ‘hatching’ and migrating/radiating into the surrounding tissue. These fibres attract attention from keratinocytes which are constantly arriving in their misguided attempt to defend the body from this infection. The core element of this ailment is a microfibre. One of these sits like a controlling nanobot at the centre of each singularity of keratinocytes. However, this organism is not only immune to keratinocytes; it has mastered control of their abilities and is also dependent on these for its own existence. These constantly arriving keratinocytes amass not so much in volume, yet in ever greater concentration. This ever strengthening shield bonds these elements into the skin and defends this organism from remedy.
This organism is not directly infectious; to become so requires an intermediate environment. This is achieved by the development of endospores that form around the anus, which when mature rise out during bowel movements and which are then flushed into the sewer where the ‘fortunate’ ones come to rest amongst H2S which is a Volatile Organic Compound that has unusual affects on biology which are not yet understood by medical science and which furthermore, is a common denominator for the last 400 years of this mystery.
Reproductive endospore
These alternative bullet-proof in appearance endospores are around 1.5mm in size and look like little peach stones that have what I believe to be a hydrogen sulphide detecting moustache. These endospores are alternative biology for the normally fibre producing endospores that I suspect alternatively form here consequent to the proximity of faeces and which then need to languish in H2S to complete MD’s life cycle and become infectious. Whereupon, mature infectious microfibres break out from within and float on the surface of this heavy gas. I took a massive direct hit, yet strongly suspect this extremophile could survive for a period of time on the ground and from there again be airborne carried on/with dust? These infectious microfibres are the 4th MD anaerobe element identified and the only one that I have not been able to objectively classify, these must be aerotolerant; however, I cannot know to what extent. Men in white coats are more than welcome to that job!
The malformed hairs, fibres and sores demand the most attention; however, it is keratinocytes that are the ‘Keystone’ issue’ with microfibres being the ‘pert/active’ ‘live’ epicentres of the MD organism, each and every one of these billions of microfibres has its own shield of hijacked keratinocytes. With brain fog regularly reported as a symptom, I can’t help but wonder where else in the body that these presently undetectable elements could be covertly accumulating?
Forget spots, boils and pimples, think Radweld!
MD and the hijacked assisting keratinocytes manifests in a multi-stratified overlapping form within the skin, each which functions like superglue in a sponge. This ailment is present in several different forms, all with a primary directive to control the level of sticky material and the size of particulates in order to achieve a binding in the skin and which is most determined at the sites of exit.
Component biological parts:
- Microfibres
- Keratin (ocytes)
- Biofilm
- Endospores for fibres
- Fibres
- Sores
- Hairs
- Reproductive endospores
- Infectious microfibres
The larger coarse ‘hairs’ are merely cherries on MD’s cake; these appear inert, attract no attention from the keratinocytes and will exfoliate during remission along with the sores they have developed in/on. These hairs and the fibres have been stealing Morgellons limelight, whilst the covert keystone culprit hijacked keratinocytes have remained ignored?
The shield of keratinocytes that is/are defending the MD infection from antibiotic remedy also produces a bio-film that is resistant to all ‘usual’ topical emollient products available. First this bio film and then the offending errant keratinocytes beneath must be ‘broken’ to facilitate antibiotics to gain ingress past/through and address the MD infection. The keratinocytes which have backed up in the skin/body like a biological traffic jam MUST be freed up and let out. The volume of this substance that has backed up will never cease to amaze. It is essential to get this moving and to keep it moving, a ‘stiff’ one finger pressing-rub helps. When you get this blockage moving steadily, it virtually fizzes away like glassy bubbles of Alka-Seltzer in slow-mo. The remedy is frustratingly slow to begin, which then speeds up towards the end and at times is not a pleasant experience, yet as MD sufferers already know, nothing about this ailment is ‘pleasant’!
It will take several months of intensive self nursing to first exhaust and then break through the bio film and then several months more to break up the keratinocytes, then several months more for the antibiotics to beat the infection and then another several months for skin to exfoliate the mission corrected keratinocytes along with their dying or dead fibres and/or microfibres cores. The concentration of keratinocytes is so immense that this must be experienced to be believed, there is so much of this exfoliated that I cannot accept MD to be merely skin deep? The keratinocytes MUST be ‘broken’ to allow the antibiotics access to this acidophiles sores and oxygen access to the anaerobe fibres and microfibres.


They sting Crunchy nut cornflake!
My abstract description of ‘getting-better feelings’; will only become fully understood by persons who subsequently, find out for themselves? As to how ‘learned from feel’ information helped me to deduce what was most likely happening in the skin and body that I live within, will again only be fully understood by persons experiencing these ‘getting-better’ feelings. Antibiotics cause the sores to switch into a defensive mode which consequently, crystallise to as hard as toughened glass or like cast iron grit, which then spring from ‘pockets’ like exploding popcorn, into forms like ‘crunchy nut cornflakes’ or miniature ‘hedgehogs’, the larger the deposit, the more tenacious it will be and the stronger the ‘sting’ when it does.
Keratinocytes whilst losing adhesion and detaching from nerves can if not managed correctly generate pain and sensations that are way beyond rational description. Somewhat random yet mostly nocturnal ‘waves’ of weakened keratin (ocytes) rising up in the skin cause a ‘purging’ sensation, and it is ‘clumps’ of ‘active’ keratinocytes that have become separated from the ‘hive’ that cause the sensations of parasitosis. Early phases of remission are the most ‘challenging’ and least rewarding.
The only thing that is required from a doctor is a repeat prescription for doxycycline or/and, should you find that remission becomes a challenge that you need help with, a doctor could maybe help ease uncomfortable sensations in the skin with diazepam or suchlike medications? I took this on the chin; however, my constitution is strong, which was fortunate because with no help offered by doctors, I had no other choice.
I also have degenerative spine disease with presently; 9 prolapsed discs, 6 pinched nerves, arthritis in every joint and a sliding hiatus hernia. The painkillers that consequently I had previously been allowed to try for these had resulted no remedial effect and looking after myself with these disabilities and MD was challenging enough without any further debilitating medication.
The hijacked and concentrated keratinocytes are extraordinarily ‘dry’, highly resistant to emollients and remarkably stubborn to hydrate. The topical emollient treatment that I ultimately found most effective was Nivea Hemp Balm. This causes the keratinocytes to first crystallise into like a sheet of glass within the skin, before then expanding into ever more and ever smaller crystals as this exfoliates. Applied from head to foot including most importantly, in the ears and up the nose, slowly breaks up the keratinocytes and gets these moving, which as it does, gradually inflates no less than a thousand fold.
MD is a gift that keeps giving, right up to its end.
Balneum Plus Cream (5% Urea) used instead of soap for bathing, applied all over before taking a long soak in the bath aids exfoliation, especially during the first half of remission. Adding 2 pints of Bicarbonate of Soda and half a pint of Epsom salt to bathwater raises the pH, magnesium and sodium in the skin which weakens the errant acidic loving hijacked keratinocytes. It takes at least an hour for this to penetrate and have effect. Adding 2 caps of Dettol to this bathing water recipe helps to soften and lift off the sores. I soaked in this brew for at least an hour, every other evening. Bathing every-other day resulted with exfoliating the most for me; however, should skin become too itchy for comfort, treat yourself to a soak in a bonus bath. Collectively, these keratinocytes weakening activities facilitate antibiotic ingress past/through the shield and help to affect a cure. Getting better is not a secret; nerves in the skin will transmit regular keratinocytes traffic-jam movement-reports.
Whether you like it or not!
……………
Archaea: (Underscored italic & bold are elements common with MD.)
Archaea is a domain of organisms. Traditionally, Archaea only included its prokaryotic members, but this sense has been found to be paraphyletic, as eukaryotes are now known to have evolved from archaea. Even though the domain Archaea includes eukaryotes, the term “archaea” in English still generally refers specifically to prokaryotic members of Archaea. Archaea were initially classified as bacteria, receiving the name archaebacteria, but this term has fallen out of use.
Archaeal cells have unique properties separating them from Bacteria and Eukaryota. Archaea are further divided into multiple recognized phyla. Classification is difficult because most have not been isolated in a laboratory and have been detected only by their gene sequences in environmental samples. It is (was) unknown if they are able to produce endospores.
Archaea and bacteria are generally similar in size and shape, although a few archaea have very different shapes, such as the flat, square cells of Haloquadratum walsbyi. Despite this morphological similarity to bacteria, archaea possess genes and several metabolic pathways that are more closely related to those of eukaryotes, notably for the enzymes involved in transcription and translation. Other aspects of archaeal biochemistry are unique, such as their reliance on ether lipids in their cell membranes, including archaeols. Archaea use more diverse energy sources than eukaryotes, ranging from organic compounds such as sugars, to ammonia, metal ions or even hydrogen gas. The salt-tolerant Haloarchaea use sunlight as an energy source, and other species of archaea fix carbon, but unlike plants and cyanobacteria, no known species of archaea does both. Archaea reproduce asexually by binary fission, fragmentation, or budding; unlike bacteria, (previously) no known species of Archaea form endospores. The first observed archaea were extremophiles, living in extreme environments such as hot springs and salt lakes with no other organisms. Improved molecular detection tools led to the discovery of archaea in almost every habitat, including soil, oceans, and marshlands. Archaea are particularly numerous in the oceans, and the archaea in plankton may be one of the most abundant groups of organisms on the planet.
Archaea are a major part of Earth’s life. They are part of the microbiota of all organisms. In the human microbiome, they are important in the gut, mouth, and on the skin. Their morphological, metabolic, and geographical diversity permits them to play multiple ecological roles: carbon fixation; nitrogen cycling; organic compound turnover; and maintaining microbial symbiotic and syntrophic communities, for example.
No clear examples of archaeal pathogens or parasites are (were previously) known. Instead they are often mutualists or commensals, such as the methanogens (methane-producing strains) that inhabit the gastrointestinal tract in humans and ruminants, where their vast numbers facilitate digestion. Methanogens are also used in biogas production and sewage treatment, and biotechnology exploits enzymes from extremophile archaea that can endure high temperatures and organic solvents.
Human methanogenic archaea are highly resistant to antibiotics, being susceptible only to molecules that are also effective against both bacteria and eukarya. Methanogenic archaea are good candidates to test for antimicrobial activity against members of this unique domain of life. Archaea are, however, susceptible to the protein synthesis inhibitor fusidic acid and imidazole derivatives. Also, squalamine, an antimicrobial agent acting on the cell wall, proved effective against human methanogenic archaea. Statins can inhibit archaeal cell membrane biosynthesis without affecting bacterial numbers as demonstrated in livestock and humans.
……………
Archaea have a variety of interactions with sulphites
Sulphites and sulphates are both sulphur-based compounds that differ in their chemical composition, uses, and oxidation state.
Chemical composition
Sulphates are made up of a sulphur atom bonded to four oxygen atoms, while sulphites are made up of a sulphur atom bonded to three oxygen atoms.
Uses
Sulphites are used as preservatives to prevent food from spoiling and discoloration, while sulphates are used to clean hair and body.
Oxidation state
The oxidation state of sulphur in sulphates is +6, while the oxidation state of sulphur in sulphites is +4.
Occurrence
Sulphates are commonly found in minerals, salts, and water bodies, while sulphites are naturally occurring and can be found in dried fruits, salad, and baked goods.
Sensitivity
People who are sensitive to sulphites are not necessarily sensitive to sulphates, and vice versa.
Furthermore, this could also explain a connection during my remission with; absent HDL (high-density lipoprotein) “good” cholesterol blood cholesterol, elevated LDL (low-density lipoprotein) “bad” cholesterol and the spike in my blood glucose level at the onset of my remission?
……………
Obligate Parasitic Extremophiles: (Underscored italic & bold are elements common with MD.)
There isn’t much information available about obligate parasitic extremophiles, but here’s some related information about extremophiles and obligate parasites:
Extremophiles: These organisms can survive in extreme environments, such as high pressure, temperature, radiation, salinity, or pH levels. They have unique enzymes, called “extremozymes”, that allow them to function in these conditions. Extremophiles are found in many shapes and sizes, and can be classified as acidophiles, alkalophiles, obligate anaerobes, or halophiles.
Obligate parasites:
These organisms have evolved to manipulate their hosts’ behaviour, which can include:
Manipulation sensu stricto: The parasite’s genes are expressed, causing the host to display alternative behaviour.
Mafia-like strategy: The parasite retaliates against hosts that don’t comply.
Exploitation of compensatory responses: The parasite exploits the host’s compensatory responses, which can match the parasite’s transmission routes.
……………
Anaerobes: (Underscored italic & bold are common elements with MD.)
Are organisms that do not require oxygen to grow and may even die if exposed to it. They can be unicellular or multicellular. Anaerobes use electron acceptors like nitrate or sulphate instead of oxygen.
There are different types of anaerobes, including:
Obligate anaerobes: These organisms can only survive and reproduce in the absence of oxygen.
Aerotolerant anaerobes: These organisms can tolerate oxygen for short periods of time, but cannot use it during respiration.
Strict anaerobes: These organisms cannot grow in the presence of more than 0.5% oxygen.
Moderate anaerobes: These organisms can grow in between 2% and 8% oxygen.
Anaerobes are important in the human body, where they play a role in the normal flora of the gastrointestinal tract. They also help prevent other microbes from colonizing mucosal surfaces. However, anaerobes can cause disease if they gain access to sterile sites.
…………….
Incorrect ‘Official’ Consensus for Morgellons Disease:
Morgellons is the informal name of a self-diagnosed, scientifically unsubstantiated skin condition in which individuals have sores that they believe contain fibrous material. Morgellons is not well understood, but the general medical consensus is that it is a form of delusional parasitosis, on the psychiatric spectrum. The sores are typically the result of compulsive scratching, and the fibres, when analysed, are consistently found to have originated from cotton and other textiles.
The condition was named in 2002 by Mary Leitao, a mother who rejected the medical diagnosis of her son’s delusional parasitosis. She chose the name from a letter written by a mid-17th-century physician. Leitao and others involved in her Morgellons Research Foundation successfully lobbied members of the U.S. Congress and the U.S. Centres for Disease Control and Prevention to investigate the condition in 2006. CDC researchers issued the results of their multi-year study in January 2012, indicating that no disease organisms were present in the samples from the individuals examined and that the fibres found were likely cotton. The researchers concluded that the condition was “similar to more commonly recognized conditions such as delusional infestation”.
Morgellons is poorly understood but the general medical consensus is that it is a form of delusional parasitosis in which individuals have some form of skin condition with sores that they believe contain fibres. Its presentation is very similar to delusional parasitosis, with the addition that people with the condition believe there are inanimate objects in their skin lesions. An active online community supports the notion that it is an infectious disease, disputes that it is psychological, and proposes an association with Lyme disease. Controversy has resulted; publications “largely from a single group of investigators” describe findings of spirochetes, keratin and collagen in skin samples in small numbers of patients; these findings are contradicted by much larger studies conducted by the CDC, which found skin samples mostly contained cellulose that came from cotton, with no evidence of infection or other causes. The CDC has recently spent a further $600.000 on a 10 year case study of 10 patients and their research claims that the skin sores seemed to be the result of long-term picking and scratching of the skin. The CDC goes on to say;”We were not able to conclude, based on this study, whether this unexplained dermopathy represents a new condition, as has been proposed by those who use the term Morgellons, or wider recognition of an existing condition known as delusional parasitosis.” The results of the CDC study have been archived. The CDC does not plan to do any further research on the matter.
……………
The CDC has been consumed by petrochemical wealth-care to become a failed healthcare organisation.
……………
Incorrect conclusion of medical science for Delusions of Parasitosis:
DSM-IV-TR defines delusions of parasitosis as delusional disorder of somatic type. Patients believe that organisms infest their bodies; they often present with small bits of excoriated skin, debris, insects, or insect parts that they show as evidence of the infection. Pimozide, 1 to 10 mg/day, has been the treatment of choice in past87–89; risperidone, trifluoperazine, haloperidol, chlorpromazine, and electroconvulsive therapy are among other treatments reported to be useful.90–92
……………
Correct layman’s conclusion for Parasitosis:
The sensations of parasitosis are consequent to Morgellons Disease and which are caused by accumulations of active keratinocytes that are surrounding a microfibre. This activity results when this/these have for whatever reason become separated from the ‘hive’ and isolated from sufficient of the errant parasitic acidophiles signal emitted by MD. These are in a weakened state of ‘flux’; their grip has been compromised and which are unsuccessfully trying to reattach and which happens mostly during the hours of darkness. These previously unexplained strange feelings/happenings were most prolific on my head and which mostly ceased when the microfibres began to rise out. The strangest of these happenings being under my eyes, here, early in remission during the most active period for the keratinocytes, whilst creaming and rubbing, I periodically found what felt like a small grain of sand under/in my skin. These items could be chased around a large area of my face with my finger, freely moving around in the skin, until eventually popping out of an unsealed follicle and becoming trapped between my index finger and thumb. Here this/these could be felt actively gripping and grabbing at the surface of my skin, like minute active burdock seeds. However, when opening my fingers to see what I had caught, nothing was there that could be seen and when closing my fingers again, there was nothing to be felt either!
(A microscope video clip of active keratinocytes is linked in ‘supportive research’; which looks exactly how this felt.)
Parasitosis is going to happen, whether you like it or not!
However, now that you know this is not an infestation of minute creatures will counteract and alleviate such misunderstandings and concerns.

It is a trap; where the mind can only go where it is allowed to go
Brain fog: Brain fog is a subjective feeling of being less aware or wakeful than normal, and is also known as mental fog or clouding of consciousness. People with brain fog may have difficulty paying attention, and may be less aware of their surroundings and time. It is notable that I found writing this dissertation to be far less taxing during the hours of darkness, with my clearest thoughts and the majority of my inspirational revelations happening just before dawn. My experience of this is maybe the most important sentence in this paper. Drawing this abstract into the open; it appears that I’m the first ever escapee and I believe that it would be more accurate to describe this abstract as like the web of a funnel web spider. It is a trap; where the mind can only go where it is allowed to go. I will not try any harder to put this abstract into words; that would only confuse the matter. I will however, add a photograph of a funnel web and let psychodermatology and medical science draw their own conclusion!
Evicting MD fibres from the brain: If you’re wondering how hemp balm gets MD fibres out of the brain? MD is an anaerobe; it must keep the skin sealed and keep oxygen out to survive. As the airtight seal in the pores is broken; consequently, these fibres which are totally impervious to antibiotics and which are the most effective MD element for attracting the attention of errant keratinocytes are best at the job of sealing the follicles, consequently, these fibres migrate back to the surface to join in with the fight to keep the oxygen out; these are secondary elements which cannot survive without the primary element microfibres and or the errant signal producing sores. Simples!
Microfibres encapsulated in their shield of errant keratinocytes are far more mobile within tissue than the fibres, however, the fibres are completely resistant to antibiotics and THC.
I believe these to be fibres, because the microfibres are ‘scared’ of THC.
I will wager a pint on it!
Like I have explained elsewhere, you need to get inside MD’s head and then turn its defences around to fool it into destroying itself. MD sneaked uninvited into yours and with this information you can now get your own back!
That’s how Psychodermatology works, even though Psychodermatologists haven’t yet worked this out.
This also explains where the billions of them magically come from!
If you can get your head around this concept, this is a remarkably powerful transferrable skill that has more uses than you could imagine! I did say at the beginning that I thought my psychology degree might come in handy. I wrote that sentence more than 2 years ago and it turns out on this occasion that it came in handy for psychoanalysing a micro organism!
It’s now 8 days without sleep; these revelations keep waking me up right at the moment of dropping off and launch me straight back into the Wide Awake Club. My brain literally works out this and/or any other stuff that I am challenged by in a microsecond when I sleep! I have up until now; had to work hard at working this mystery out, which is the first time that I have had to do so in my life, but now that my brain has been freed and is back to normal for me, I spend the days writing down the answers whilst my mind does the working out when I’m asleep. Not showing my workings out has got me into trouble more times than I can remember?
The pen is mightier than the cane when the brain is mightier than the pen!
It’s the preceding unmentioned second half that’s the important bit.

Contents of a fibres producing endospore
Biofilm: Biofilm is this acidophiles influenced product of the hijacked keratinocytes and is just one of the many forms that keratinocytes can take. This transparent film is impervious to usual emollients; hemp balm however, is an exception to this rule when used in conjunction with the bathing recipe. Biofilm is MD’s first line of defence; nevertheless, this I turned around helping MD to defeat itself. The hemp balm constantly neutralises this biofilm and MD constantly replaces this at its deficit. This first stage of remission may go on for several months until MD’s ability to keep up is exhausted. From here on in, the hemp balm will begin working on keratinocytes within the skin.




Crispy On the Move Properly on the move Keratin with Microfibers
Keratinocytes: (Acidophile influenced)
These acidophile influenced keratinocytes are The Keystone Issue, the cause of parasitosis and are the most challenging element to describe.
It’s your job to clear these. Your prime directive is to “help the dogs to find the rabbits” by means of encouraging this/them to ‘decompress’ which gradually weakens the shield and which ultimately, then allows the antibiotics to get at the sores and do its job and for oxygen to get at the fibres and/or microfibres. MD literally team-fights in its efforts to keep the follicles sealed and keep hold of the keratinocytes. When MD’s grip is strong, this holds Keratinocytes in an overlapped and glued ‘locked’ formation in the skin. I have explained elsewhere how to unlock this.
THC purges keratinocytes towards the surface where this can and will mechanically grab and grip at the points of exit. Moisturising and rubbing breaks this grip and keeps it moving.
As the infection weakens this purging weakens too, yet the good news is, copious moisturising will now hydrate the keratinocytes which are exfoliated from the follicles as if dead skin. Getting keratinocytes moving up and out and keeping them moving up and out is the route to becoming cured.
This stuff is like shape shifting Swiss Army knives that can and will take many and any forms and/or whatever variation of forms which most efficiently locks the skin. These transformations take place in the blink of an eye.
When the keratinocytes have been exfoliated and the grip consequently exhausted and no longer functioning, from every follicle, a bundle of fibres then gently fluffs up and rises out, some immediately, like popping popcorn of little rubbery sponges, others slowly like balls of dead skin and hat felt fibres.
All of these things are going on in the skin and you can feel all of these things going on.

Keratin oozing out looks like fast growing cress!
Informed of these strange happenings and with understanding of what is causing these feelings and/or sensations means that you can stop worrying about them.
However, that won’t stop you being pissed off about it; that’s the way it is; just learn to accept it.
Different parts of the body will have different behaviour.
The strength of the infection can be monitored by the activity of the keratinocytes whilst rubbing.
The finer these crystals become the closer it is to its end. Remission is not a pleasant experience and we all have different abilities with tolerance and each will have a differing maximum for the level of ‘purge’ within their tolerance. Getting better is good, yet it’s possible to have too much of a good thing. Progress is a ‘biorhythmic yoyo which is under your control/influence. I never achieved what I would regard as ‘full control’, nevertheless, by administering ‘full influence’, remission can be maximised.
Don’t be complacent by thinking that one follicle partially cleared here and there is a futile exercise when there are nearly 4 million to go. These; one here and there partially emptied follicles inexorably allow the Hemp Balm to penetrate deeper into the skin which translates into a patch of skin here and there which allows in oxygen which is what kills the anaerobe fibres and eventually this joins up.

(Zoom in) Keratin (ocytes) migrating up hair
Remission progresses in the manner of an all over rising. This is not obvious, because there is often/always one place on the body that is far more active than others and which commands attention in more ways than one. MD has terraformed the skin, if not the whole body into its own world with its own environment. This ‘world’ has an Achilles heel, a weak spot like a hole in an ozone layer, which reveals itself somewhat randomly, anywhere from head to foot, you never quite know where, yet always with symmetry. First THC after 4 days without and you will find out where this is to be in about 7 minutes? Which rarely happens where you might expect, for best results, follow this wandering weak spot during peak waves with extra creaming and/or rubbing. Remission literally is a ‘decompression’ of MD’s World. When this ‘environment’ has been completely released.
MD will have been released with it. And you are cured.
Form/colour/consistency not dissimilar to skin, it’s ‘degeneration’ however, involves a sequence of ‘crystallisations’, first to like putty, then to like glass, then to like sand, then to like peach fur, then to like latex rubber then to like dead skin, with ‘liquid-glass’ bio film replacement at all stages. This activity entails, ‘thousand fold’ expansion, not as increased volume, but as replacement. It is important to keep it loose and moving/exfoliating with rubbing, if this is allowed to backup and get back up to ‘pressure’ it’s grip and tenacity regains strength.
When the keratinocytes have been broken sufficient for the antibiotics to get through, the infection retreats into a glasslike state of self preservation that takes the antibiotics and or bicarbonate of soda several months to eliminate.
The keratinocytes begins to rise up and out like hollow glass cones, in patches/areas instead of individual follicles which quickly degenerate to first like sand, then to like peach fur, then to like liquid metallic glass, before disappearing as if it was never there!
The keratinocytes enter the follicles from the sides, above the fibres to protect these from oxygen.

Analogy for keratin (ocytes) in skin
Flat-bubbles, stratified, and deepest largest.
The keratinocytes I suspect are trapping a hydrogen sulphide element? Not just the smells, but the metallic appearance, like the interface when H2S floats on water?
White or translucent malleable inside, grips at exit.
Keratinocytes are exceptionally busy and remarkably determined with their own set of rules and many guises, that includes descriptions such as; biofilm, locked, unlocked, glued, bubbling, sheet glass, glass-shards, micro-glass bubbles, peach hairs, fizzing, grabbing, spraying, latex-balling, flowing, crystallizing, crispy-honeycomb, moving, sand, peach-fur.
Switching between any, each and or all of these manifestations in the blink of an eye before eventually; disappearing as if it was never there!
This is a yin & yang battle between the errant MD signal and the ‘normalising’ effect of the bicarbonate of soda, hemp balm and THC resulting with the keratinocytes receiving less of the ‘errant-signal’ than is originating from the sores.
An unimaginable volume of highly concentrated keratinocytes inflate/expand and/or ‘decompress’ out from/through the skin, which gradually/eventually and at increasing speed, disappears into nowhere?

More than this; every day for over a year!
I am certain that this “Swiss army knife” “shape shifting” activities list is not all encompassing; there is certainly no shortage of variety.
The volume of keratinocytes to be exfoliated will far exceed any expectation you may have. MD’s defence is acidification and dehydration; balance pH, moisturise & rub, moisturise & rub and moisturise & rub.
Keratinocytes may have accumulated in compressed form to covertly become around 50% the volume of skin and which gradually inflates 1000+ fold before it is gone, with the deepest deposits being the largest.
Some eject their core, yet the remainder is like pieces of toughened glass which slowly grows up & out.
There are vast quantities in the skin that ‘comes out of hiding’ and rises to the surface in a ‘from another dimension’ kind of way?
Skin plumps up, the follicles dilate and skin is in ‘unlocked’ mode.
Keratinocytes grabs at the point of exit and seals the follicle and skin is then in ‘locked’ mode.
Deepest in ears, most prolific around base of scalp, most glasslike on top of scalp and between the eyes and ears, most stubborn on protruding parts, cheek bones, ear lobes and eyebrows, most painful on scalp and actively determined on head & groin.
Should I have kept everything that has risen up out of my skin, there would be enough to fill several buckets.
The keratinocytes deposits do not amass in volume, but amass in concentration as if ‘singularities’, this first crystallizes from like rubber to become like glass, followed by crystallizing to like grains of sand, followed by then crystallizing to like peach fur, before eventually hydrating to a thick paste, which inflates a thousand fold, thankfully not in one go, yet over time gradually fizzes away from the periphery of each deposit. Up until its hydration Grand Finale, this active substance grips, grabs and adheres to the inside of the follicles right at the point of exit. When skin is in ‘unlocked mode’ moisturising and rubbing keeps this moving, however, when skin reverts to ‘locked mode’, no amount of encouragement is capable of shifting this. The hydration Grand Finale combines with losing this ability to grip. The keratinocytes are most determined to encapsulate the fibres and microfibres; however, the driving force for this originates from the sores. Regardless of how often the keratinocytes are exfoliated, these are instantly replaced. It may seem as though it is coming from a bottomless pit and that this will go on forever, nevertheless, every time that this expands to fill the vacant space, it becomes weaker until these ‘singularities’ eventually run out and oxygen will then come into contact with the fibres and then they are dead.
The follicles are ‘fed’ from their sides and become perpetual keratinocytes ‘plugs’ with many anchors.
In the beginning, these ‘go off ‘one at a time, mostly independent of others, like a bubble-wrap made up from millions of singularities. Eventually, antibiotics will reduce the influence from infection over the keratinocytes and then; the all over Great Rising begins! The keratinocytes expansion is slow and steady and which only inflates to replace space/pressure from lost keratinocytes. The infection however, which although inflates far less, when the antibiotic gets to it this can do so in short time and which can be uncomfortable. Last but not least, the billions of fibres rise out of the skin dead like little balls of hat-felt and the microfibres, alive until contact with oxygen within the last of their keratinocytes shield.
Microfibres: These anaerobes are the core element of this ailment; there were billions of these which can follow alternative biological pathways to develop into sores, endospores for fibres or endospores for infectious reproduction.
Notably, in the exact same places where I had the massive keratinocytes response at the moment I contracted this. At the site’(s) of original infection, these exist in colonies where they reproduce by binary fragmentation or maybe fission? Excuse me; my eyesight is not good enough to be sure and this only happens out of sight inside the skin where it’s isolated from the oxygen in the air. During which time keratinocytes are constantly arriving which keep the follicles sealed airtight.
Within this colony, a slight positive pressure develops within the air tightly sealed skin, which then transmits these microfibres to other parts of the body by osmosis. Over time, MD develops pathways in the skin like arteries. On my head against the skull these could be clearly felt and/or seen laid out like a road map. Each and every one of these has its own active ‘shield’ of keratinocytes and when one finds an unpopulated follicle; it claims this for itself and develops into an endospore to develop fibres, sores or infectious reproduction.
Most prolific in and around my ears, eyes, scalp, eyebrows, cheeks, jaw line and nose, my knees were a site of original infection too, however, here there was far less proliferation. It appears that the microfibres require a moist area to proliferate.
From these sites, they migrate around the body in their own highways similar to veins, where on the head against the skull, these can be clearly felt and/or seen laid out like a road map. There is no open thoroughfare within; nevertheless, this biology migrates through the skin as if it was not there. Each one then lays claim to a follicle where it subsequently develops into an endospore for fibres or sores.

Microfibres route way
During remission, these microfibres rise up in the skin ‘pert’, each with its own protective shield of active keratinocytes which then ‘sinter’ to become like an army of little soldiers tightly packed shoulder to shoulder in the skin, like reed mace seeds, which are revealed around the eyes looking like a bruised ‘black eye’ consequent to them now being viewed collectively from their ends. Each & every one of these is coated with active sticky keratinocytes and which are all ‘holding hands’. These microfibres are anaerobes that can’t survive without keratinocytes to protect them oxygen and these rise and/or rub out when their defensive shield has been exhausted and/or sometimes these can ‘skip’ out with the very last of the keratinocytes around them whilst still pert. These began rising around 6 months after the fibres and continued until the end. There are nearly four million follicles which all need your help.

Black eye Keratin with Microfibers
As the shield of errant keratinocytes are exhausted, these microfibers will rise up and there are far more of these than could be imagined, however, these will not die from oxygen exposure until the moment of exfoliation.
The larger secondary fibres are less oxygen tolerant and their strategy is to exist within a greater shield of hijacked keratinocytes.

Puncture repair patch
Sores: These acidophiles are a secondary development from a microfibre that without doubt is another alternative biological route for an endospore; the redundant largest hairs amongst the sores are evidence of such. For me, I had no sign of sores whatsoever until I started taking the antibiotics, which I deduce to be indicative of the strongest variant of MD. Most prolific on scalp, shoulders and biceps, with a random yet symmetrical spread across the whole body, yet notably none on my back. These were shallow and broad over bone; however, grew deeply where over soft tissue with the largest deposits over and penetrating into large muscles, which go-off like little time bombs. The worst areas for stinging are indicative of the areas with the most covert sores. This obvious symptom may not be otherwise be apparent, until later in remission. These events are sooner or later followed by the rising up and spreading out of large ‘sores’ and these will continue on right until MD’s end.
These respond to the antibiotics by turning into a defensive form as hard as toughened glass, before then exploding like popcorn, into shapes like a crunchy nut cornflake or a miniature hedgehog. This stinging activity begins around 2 weeks after taking the antibiotics? Presently, this is referred to as ‘die-back’, but there’s not much dying going on. This is MD responding by punishing you, trying to persuade you to stop taking the antibiotics.
In the beginning there are a lot of these, which over maybe a year become much fewer yet are ‘stronger’ because these are larger and/or have a greater volume of keratin (ocytes) around and beneath them for their protection.

Keratin rising from beneath a sore
Nevertheless, these strange sores are not sores at all. MD is an anaerobe which is why it keeps the follicles sealed closed. Pockets of this ‘infection’ develop deep inside a follicle that is sealed with a keratin plug at the exit. When for whatever reason this plug is exfoliated, this allows oxygen to contact the infection. This element of MD is the most tolerant of oxygen and will respond by defending itself by repairing the open follicle with an airtight patch. A red substance will rise from a single follicle, then spread out into a circle and set to as hard as toughened glass, as this dries it bonds to the skin like a bicycle inner tube repair patch. It might not look like it; however, rising sores are a sign of remission. Every time this pocket has to repair itself, is at the expense of the volume of archaea infection in the follicle. The base of this infection is protected from antibiotics by keratin (ocytes). Regular application of Hemp Balm causes the keratin (ocytes) to rise up and out around the edges of the patch. The more of this that rises out, the less protection it has underneath and the more effect the antibiotics will have. Picking at these results with nasty scars and are best left alone. However, soaking in the bath recipe will soften these, which after around an hour, then turn green, shrivel up and fall off without leaving a mark. An hour or so after bathing, another will/may rise out and form. Just let it get on with it, that patch will get nailed during your next bath. This will continue repeating until the pocket has been exhausted and is gone. The last of which does not raise a patch, this changes tactics to stay crystallised and which bonds itself into the follicle as is by superglue. Nevertheless, this leaves the follicle open and the bicarbonate of soda will then defeat this acidophile, one bath at a time until it is gone. It is not noticeable until later in remission, however, it is these pockets of infection that are producing the acidophiles hive control element that influences the keratinocytes. MD’s ability to do so is not impeded by this defensive crystallisation. Each pocket radiates an influence on the strength of the keratinocytes around it. The fewer the pockets there are and the further away, the weaker the keratinocytes bond. The fewer the sores, the weaker MD becomes.
Soaking in the bath recipe is an essential part of this cure, because this turns MD’s defences around to beat itself. The more sores that can be soaked off the more MD has to replace the patch at its own expense until the pocket is exhausted. When you think these sores that at not sores are bleeding, you are actually getting better, if when these ‘bleed’, you can encourage this with gentle rubbing, these can beaten in less time. The largest one of these on my body was in my left eyebrow and I didn’t even know it was there until the Grand Finale! Don’t do picking and squeezing, just a gentle rub to clear the risen infection before it sets into a ‘toughened glass’ bicycle inner tube patch and MD will respond by sending up some more to try again. Learn the gentle art to do this and then without causing any pain the largest deposits can sometimes be emptied completely in a couple of days. Again, this turns MD’s frontline defence against itself. Never forget that you are your own physician, there will never be a doctor next to you when you think that you need one. The reality is that you don’t. You literally defeat each and every component of this organism with Psychodermatology. You need to learn how to out think MD.
Study every single word in this document until you are sick of looking at it!
You will not be able to beat MD until you learn how to get inside of its head. The sooner that you can get your head around this the better; the more that you learn about MD, the less bothered by MD you can/will be. All that you need to do is to become a better psychologist than an organism that medical science hasn’t/can’t yet found/find! However, please don’t tell this to a doctor until after he/she/it has read this; or before you can say Jack Robinson, you’ll be awarded a Green Shield stamp for psychosis!
Contents of a fibres producing endospore
Fibres: These anaerobes form inside endospores and are a secondary element that can be any or many colours and which appear to remain the same size as when they hatch. As keratinocytes are released from the skin, these fibres retreat back to the follicle and form into like little balls of hat felt, ultimately rising out limp/dead inside a ball of glue along with the last of the keratinocytes. These will tell you when they’re ready and rise out with the lightest of touch. Sometimes one of these is stronger lived and can hang on for longer than the keratinocytes glue, without which, this ultimately twangs out like a little coiled spring. For me, this began after a year and which increased until the end. Contact with oxygen is their nemesis; these MD components are the least resistant to oxygen, which is why they are protected with/by the most keratinocytes.

The most impressive “hair”
Hairs: Develop on/in sores. These largest ‘fibres’ appear to be inert, attract no attention from the keratinocytes and exfoliate along with the pockets of crystallised infection beneath the ‘sores’.




Preparing to hatch Hatching Hatching Failed endospore exfoliated
Secondary fibres endospores: These little kidney bean shaped sacks exfoliate broken after the fibres have hatched. The keratinocytes have no attraction to these at all. After the fibres have migrated into the surrounding tissue, these exfoliate quite early in remission looking like little pieces of broken eggshells.

Reproductive endospore
Infectious reproductive endospores: Formed only around the anus, before then exfoliating and migrating to lesser-fresher pastures seeking H2S to mature. I suspect that proximity to faeces could trigger this alternative biology for these endospores? It was previously unknown to medical science that archaea are able to produce endospores.
Sores endospores: I have never seen one; however, I have no doubt whatsoever that these exist too, everything else is generated in an endospore and which includes fibres. I suspect these as yet to be seen endospores are an alternative biology that results with acidophile sores, the large hairs that are found amongst these confirms this.
……………
Morgellons Disease Proliferation on Body, listed from head to foot:
Entries to within the body: For an ailment that is supposedly a skin complaint, MD has greatest concentrations around entries into the body. Eyes, ears, mouth, nose anus and navel, the tip of my penis was spared, however, that is not the case for a vagina?

GET YOUR HAIR CUT!
Hair: MD is most prolific and resilient beneath hair; consequently, I recommend a regular no.1 cut of all body hair; there are plenty of wigs or hats to choose from if you must.
The longer the hair, the greater the handicap for the creaming and rubbing that is essential. Cutting hair is crucial and which is also a psychodermatological challenge that leaves you with ‘nowhere to hide’.
This is an acid test for tenacity and power of will.
If you do not or cannot exercise this control over your body hair, you cannot and will not beat MD!
This is just one of the personal challenges I have identified which includes less obvious and discreetly ‘hide able’ factors like drinking of sufficient liquid and/or applying sufficient hemp balm. These obscure and abstract yet crucial factors, now exposed have nowhere to hide.
Head: A site of initial infection, mostly consisting of microfibres with secondary developments of sores to feed the errant signal and is most determined here. Secondary fibres developed inside ears and around nose, which were also surrounded and additionally reinforced with/by microfibres each within their own shield of keratinocytes and which cements MD’s strongest claims around entries into the body. Developing like a road network that could both be felt and seen on the scalp and which accumulated in volume on back of head under hair with high density concentration over gristly areas; nose & ears. Everywhere on my head was ‘special’, crown of scalp for tenacity, around my eyes (spectacle form) for volume of micro fibres, with my ears being the most ‘special’ for being virtually bottomless pits. Cheekbones and jaw line were special too; each part of my body experienced remission with alternative ‘character’.
Scalp: The most tenacious microfibres inhabit here, my scalp was covered with MD’s pathways, like a road map of central London. Keep the scalp well moisturised with hemp balm, I recommend once every hour.
Neck: The pathways that MD formed from the head which was the most prolific site of original infection, then all run down the neck on their way to fresh real estate lower on the body. Resulting with prolific amounts of secondary infection fibres where there were multiple colonies in each follicle.



Lots of sores Swelling & earache Keratin purging
Ears: The most challenging place on the body and the only place where there were painful swellings. These were quite regular and were most challenging. MD fibres and their surrounding keratinocytes & microfibres had penetrated deep into my inner ears and the expansion that takes place during remission causes earache. Fortunately, these deposits ‘go-off’ one at a time, unfortunately, this means earache is a regular occurrence. I was often hard of hearing and occasionally deaf. Ears are like bottomless pits. Earache is yet another tactic of MD to punish you.

GRAND FINALE!
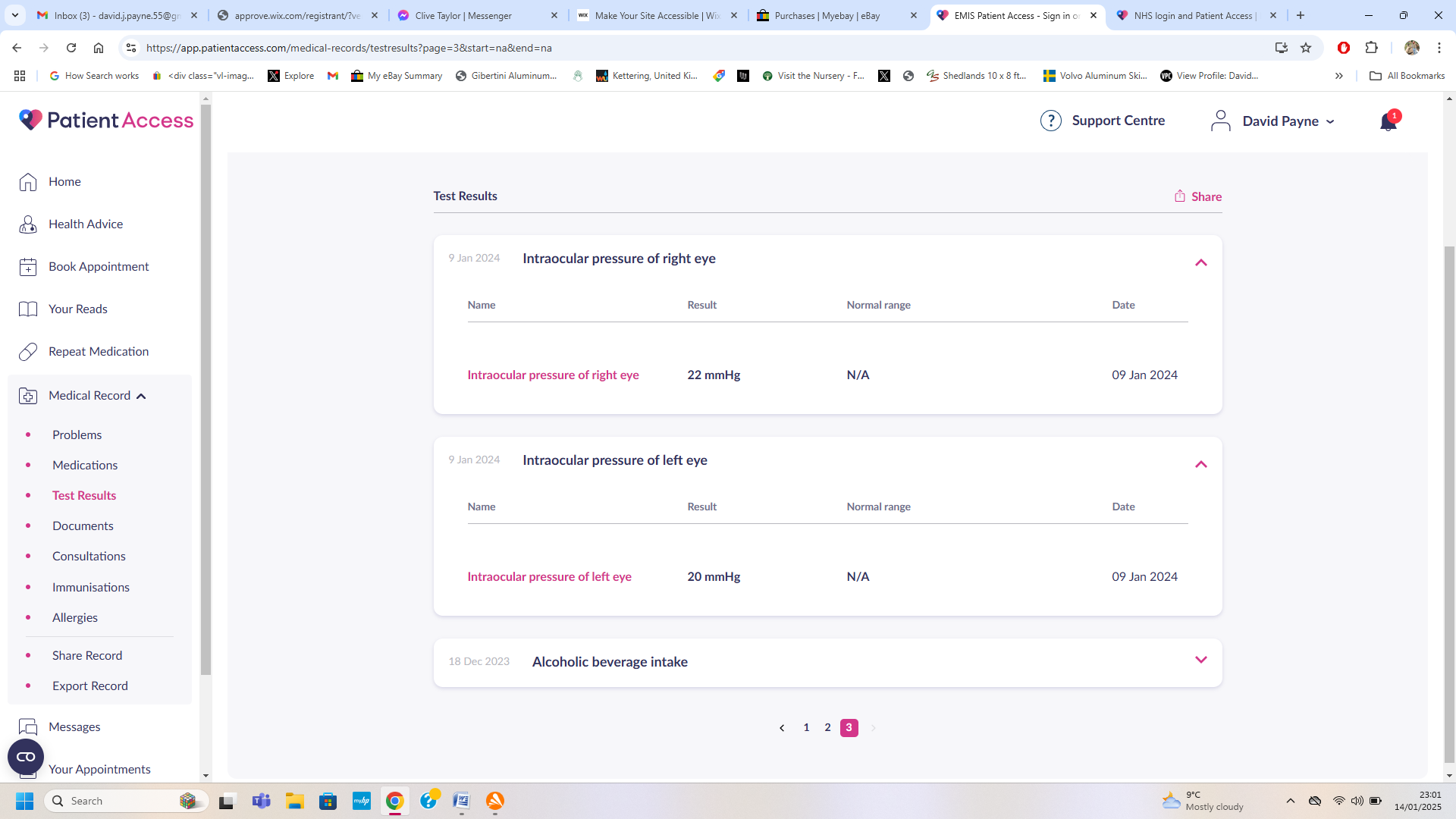
Eyes: Microfibres are prolific and tenacious around here and the second most challenging place on my body, even though this was not revealed until the eleventh hour of remission. Once remission began in earnest, expanding keratin (ocytes) around my eyes resulted with high eye pressure readings consequent to the misshaping of the eye sockets which caused the shape of my eyes to vary and which resulted with my focal length altering by more than a foot during the course of each day, this began during the second year of remission and which continued until the end, with this being at worst first thing in the mornings. Whilst expanding in my eyelashes, these could be felt pressing onto my eyes. Be aware that this symptom could be misdiagnosed as glaucoma, which my doctor associated with type 2 diabetes which I definitely do not have and my refusal to play his futile box ticking diabetes games was a constant source of ridicule. In fact after my final consultation, the graph that showed the spike indicating the beginning of remission, magically disappeared from my medical records? During later stages of recovery, as micro fibres lost their shield of keratinocytes, these rose up to the surface where they ‘sintered’ together over and around my cheek bones, standing up like little soldiers, all packed together like reed mace seeds working as a team with their last ditch effort to remain anchored in the skin. This eventuality appears as if this were a pair of bruised black eyes.
Please note: this consequence made it ‘challenging’ to be able to focus on the screen to record these details and was another obscure means of MD punishing me. During the second year of my remission, I could only drive my car in the afternoons when my eyes were back into focus for distant sight.
Eyebrows: A most prolific and tenacious place, prime real estate under hair, and it is the Beverly Hills for MD here, microfibres, fibres and sores. Keep well moisturised, this will most probably be the site of MD’s last stand?
Eyelashes: A proper wind these are; secondary fibres protected by microfibres and prolific with sores too. These can be felt pressing onto the eyes when your head is on a pillow. The sores here are larger than you could think possible, which because is a naturally well hydrated area cannot reseal the follicle. Consequently, when these ‘go off’ they will empty in one event. This looks as if your eyes are bleeding; there was so much of this it dripped off of my chin. Don’t worry about this, it is painless, just think yourself lucky that these clear in one event and do not reform.

The Biggest & deepest ‘sore’! – 2 years to empty this one!
Nose: Inside prolific with microfibres, outside prolific with secondary fibres. The tip of my nose was discretely the site of the second largest sore on my body; this one took around 2 years to completely exfoliate.
Under Eyes: The most prolific place on the body for microfibres, around the eyes is the most tenacious place on the body where MD will make its last stand.
Inside mouth: Microfibres and sores. There were 5 sores in my mouth, I lost a tooth for every one of them. Taking calcium supplement prevented further loss. MD appears to rob calcium from the bone around tooth sockets. Inside my mouth was the first place to clear, after several months of feeling the microfibres on the roof of my mouth with my tongue.
Lips: No fibres here, just micro fibres and sores. These don’t erupt through the lips, these rose from the first adjacent line of follicles in skin which penetrate and populate deeply into the entirety of the lips. Here, due to this being a naturally hydrated area, same as with anus, these sores cannot take crystallized form, which allows the antibiotics to get on with their job. You won’t even know this is going on until a large plug of keratin rises out, shortly followed by the dead sore which exfoliates like a black slug.
Jaw line: Prolific with microfibres, no secondary fibres here. Very tenacious area; keep well moisturised and leave well alone. The only place on the body that was itchy. Keeping my facial hair to a number 1 cut allows for moisturising sufficient to keep it calm.
Anus: Take good care of your anus, the groin is one of the most tenacious areas on the body and there’s a lot going on down there. After a bowel movement, wiping with toilet paper is not enough, I also used flushable wet wipes, which gets into the nooks and crannies and also helps to exfoliate the endospores before these start burning. Always give this a good creaming up when done whilst there. Notably, anus & lips were the only places that the sores did not crystallise. Alternatively, these behaved more like a ‘normal’ infection, albeit a very tenacious one, I suspect because the skin was more hydrated in these areas? Here, the sores eventually die in situ, announced first by a plug of keratin (ocytes) rising out, shortly followed by the dead infection that slides out looking like a small black slug. The developmental endospores for the fibres behave differently here too; these exfoliated before or during hatching and here is also the site where the infectious endospores develop. When either of these begins to rise you will know about it because this is accompanied with an itchy and burning sensation, nevertheless, a generous application of hemp balm and a gentle rubbing easily brings these offending items up and out. Sores and the largest fibres endospores and reproductive endospores prolifically form here. These components exfoliate onto your fingers and from here can be collected the best biological samples. When you start catching Salvador’s, do the world a favour and destroy these with fire. That is unless medical science has woken up and wants a few Salvador’s to play with? Don’t expect much traffic from here until the second half of remission.
Buttocks & Legs: Large muscles in these areas attract large sores that penetrate deep into the muscles, on both thighs and calves. Consequent to their size, these will be most tenacious and repeatedly sealed. No special treatment required, just be consistent with the treatment and be patient.
Knees: For me, these were a site of original infection where there were microfibres only and no fibres. These microfibres were discreet yet most tenacious here.
Navel: MD regards the navel as an entry into the body and here also develops the largest fibres endospores. Don’t pick and poke about here, just keep it well moisturised. There is a huge amount of keratinocytes to come out of here.
Feet: The furthest place away from the sites of my initial infection and consequently, here the infection was least advanced. No sores, just secondary fibres, with the least proliferation of keratinocytes.
Shoulders and Biceps: Sores and secondary fibres were prolific here, large and deep.
Forearms: A site of original infection, microfibres and sores only and prolific with tenacious keratinocytes.
Hands: A site of original infection; where microfibres were discreetly the most prolific on the body, no sores and no secondary fibres.
Back: No microfibres and no sores, just secondary fibres and keratinocytes.
……………
Notable similarities with another previously unidentified autoimmune ailment
Keratosis Pilaris: (Underscored italic & bold are common with MD.)


MD waxing looks like KP MD waning looks like KP
Is regarded by medical science as a harmless skin condition, which can’t be cured or prevented and which affects probably half the people on the planet. Also referred to as follicular keratosis, lichen pilaris, or colloquially chicken skin, is a common, autosomal-dominant condition of the skin’s hairfollicles that medical science has mistaken as genetic. This is characterized by the appearance of possibly itchy, small, gooseflesh-like bumps, with varying degrees of reddening or inflammation. It most often appears on the outer sides of the upper arms (the forearms can also be affected), thighs, face, back, and buttocks; KP can also occur on the hands, and tops of legs, sides, or any body part except glabrous (hairless) skin (like the palms or soles of feet). Often the lesions can appear on the face, which may be mistaken for acne or folliculitis.
The cause of KP is not (was not previously) understood. As of 2018, KP is thought to be due to abnormalities in the process of depositing the protein keratin in hair follicles, abnormalities in the hair shaft, or both. KP is usually diagnosed by a medical professional based on the appearance of the skin, but dermoscopy can be used, as well, if the diagnosis is unclear. Variants of the ABCA12 gene have been associated with KP.
KP is the most common disorder of the hair follicle in children. How common it is in adults is unclear since keratosis pilaris is an underreported condition and the actual prevalence of the condition may be higher than estimated. No single approach has been found to completely cure KP, but treatments can improve the cosmetic appearance of the condition. Treatment includes the application of topical preparations of moisturizers and medications such as glycolic acid, lactic acid, salicylic acid, urea, or retinoids to the skin.
Signs and symptoms
KP results in small, rough bumps on the surface of the skin. They are skin-coloured bumps the size of a grain of sand, many of which are surrounded by a slight pink colour in light-skinned people and dark spots in dark-skinned people. Most people with KP do not have symptoms, but the bumps in the skin can occasionally be itchy. Irritation due to scratching KP bumps can result in redness and inflammation.
Though people with KP experience the condition year-round, the problem can become exacerbated, with the bumps likely to look and feel more pronounced in colour and texture, during the colder months, when moisture levels in the air are lower. Increased sun exposure might mitigate the symptoms of KP.
Whilst MD was waxing it passed through a stage looking just like keratosis pilaris, yet progressed to become all joined together and the same again in reverse whilst waning. With around half the people on the planet having KP at one time or another, I suspect consequently that pathology tests ignore this organism which has been accepted as ‘normal’ to be found? Nevertheless, the reason the keratin (ocytes) are there is because an infection is present. I mentioned this more than 3 years ago, however, I was ridiculed by ‘those who thought they knew better’; however, I can now show my working out with 2 photographs.
There is (was) currently no known cause or cure for KP.
I strongly suspect this is the same archaea organism as MD which has matured amongst lighter heavy gasses.
Fibromyalgia: (Underscored italic & bold are common with MD.)
Fibromyalgia is a chronic condition that causes widespread pain and tenderness in the body, along with other symptoms; fatigue, trouble sleeping, headaches, lower abdominal pain or cramps, depression, insomnia, hypersensitivity, cognitive symptoms, dry eyes, and rash.
Fibromyalgia Symptoms and Complications
The pain can range from mild to severe, and may be worse in the morning and evening. It can affect any part of the body, but often starts in the neck and shoulders. Pain may worsen with activity, cold or damp weather, anxiety, and stress.
There’s no cure for fibromyalgia, but treatments can help manage symptoms. These include: exercise or other movement therapies, psychological and behavioural therapy, medications, and relaxation and stress-reduction measures.
To diagnose fibromyalgia, a doctor will take a medical history and perform a physical exam. They’ll look for widespread pain throughout the body for at least three months.
The cause of fibromyalgia is (was previously) unknown, but researchers believe it may be linked to sleep problems, stress, immune system, endocrine, or biochemical problems. It may also be genetic, (no it isn’t) with people who have biological parents with fibromyalgia being more likely to develop it themselves. (this is an environmental factor only) There is currently (was previously) no known cause or cure for Fibromyalgia. (I strongly suspect/believe that this MD cure programme could/would also cure Fibromyalgia?) I strongly suspect this is the same archaea organism as MD which has matured in an alternative recipe of heavy gasses, including methane?
Lyme Disease: Lyme disease is an illness caused by borrelia bacteria. Humans usually get Lyme disease from the bite of a tick carrying the bacteria.
Ticks that can carry borrelia bacteria live throughout most of the United States. But Lyme disease is most common in the upper Midwest and the north-eastern and mid-Atlantic states. It’s also common in Europe and in south central and south-eastern Canada.
You’re at risk of Lyme disease if you spend time where the ticks live, such as grassy, brushy or wooded areas. Taking safety measures in these areas can lower the risk of Lyme disease.
I deduce that the connection incorrectly perceived between Lyme disease and Morgellons disease to simply be consequent to these pathogens being prevalent in the same region/environment.
……………
Subject specifics in alphabetical order:
Allergies: Identifying Morgellons Disease as an Archaea infection, I believe explains my consequent nasal reaction ‘allergy’ to the smell of garlic preserved in Sulphite; Sodium Benzoate. Notably: My sinuses also became allergic to mildew.
Antibiotics and archaea: Medical science may claim that antibiotics are not affective against archaea. What they haven’t worked out; is this is because the archaea is protected by hijacked keratinocytes through which the antibiotics cannot pass. Nevertheless, they will manage to get the job done in a couple of years if you help the antibiotics to get at it by removing the keratinocytes to allow access with use of the hemp balm. In practice however the archaea actually migrates towards the surface trying to reseal the exit and/or escape from the antibiotics beneath and more infection may be exfoliated than will be directly killed.
Archaea; Variety appears to be the Spice of Death:
From the early days of; 2 weeks prescription of pills, resulting with sores rising, which stopped and cleared up when the antibiotics stopped and then going back to the doctor for more pills when there were no sores whatsoever to be seen. Doctors are accustomed to prescribing antibiotics for visual evidence of infection then stop when the infection cannot be seen. However, with this complaint it’s the exact opposite, especially in the early stages of remission for MD in its strongest form, when sores are signs of remission and clear skin is a sign of strong infection.

Result from Amoxicillin
Flucloxacillin and Amoxicillin both had affect. The Flucloxacillin caused sores to break and a peak in blood glucose, so that definitely upset MD. The Amoxicillin rose less sores, however this antibiotic purged really hard and made the whole slab of keratinocytes and skin ‘float’. This infection is more intelligent than most doctors and can without doubt quickly adapt to resist regular medication. ‘MD’ is most definitely an appropriate definition. However, variety most definitely keeps it guessing and I recommend this tactic should be tried. However, suggesting such a concept could have earned me double Green Shield stamps?
Apparent Coprolalia: If you don’t already perform this, I predict that during remission you will, especially whilst rubbing your ears. As I live alone this didn’t matter, however, should you live in a family environment such things may be different? My most regular ‘involuntary’ exclamations were; “Good God!” “Fuck Me!” or “Just Get Out!”
Battlefront: Creaming and rubbing is a war to release MD’s grip from keeping the follicles sealed. This ‘war’ will be fought with many battles, making no ground during daylight and gaining ground when it is dark. MD’s weaknesses I have revealed elsewhere in this document; when these imperfections are coordinated successfully, you can exhaust MD from vast amounts of errant keratinocytes. Initially only when it is dark, however, later in remission when MD has become sufficiently weakened, this can also be encouraged during daytimes.
Biofilm: Is produced by the acidophile influenced keratinocytes and is MD’s frontline defence against hydration and oxygen. Neutralising this with the hemp balm forces MD to replace this at its deficit, this activity turns MD’s frontline defence around and helps MD to destroy itself.
Blood: When remission began in earnest, my glucose level spiked before then returning to normal parameters, then towards the end, my cholesterol levels reduced. Be aware if this should happen to you or you could easily be misdiagnosed with Type 2 diabetes. This symptom and also the resulting eye pressures are presently misunderstood by doctors and which tick the right boxes for the wrong reasons for doctors to declare type 2 diabetes.
Spike in blood glucose resulting from Flucloxacillin @ 2,000mg per day
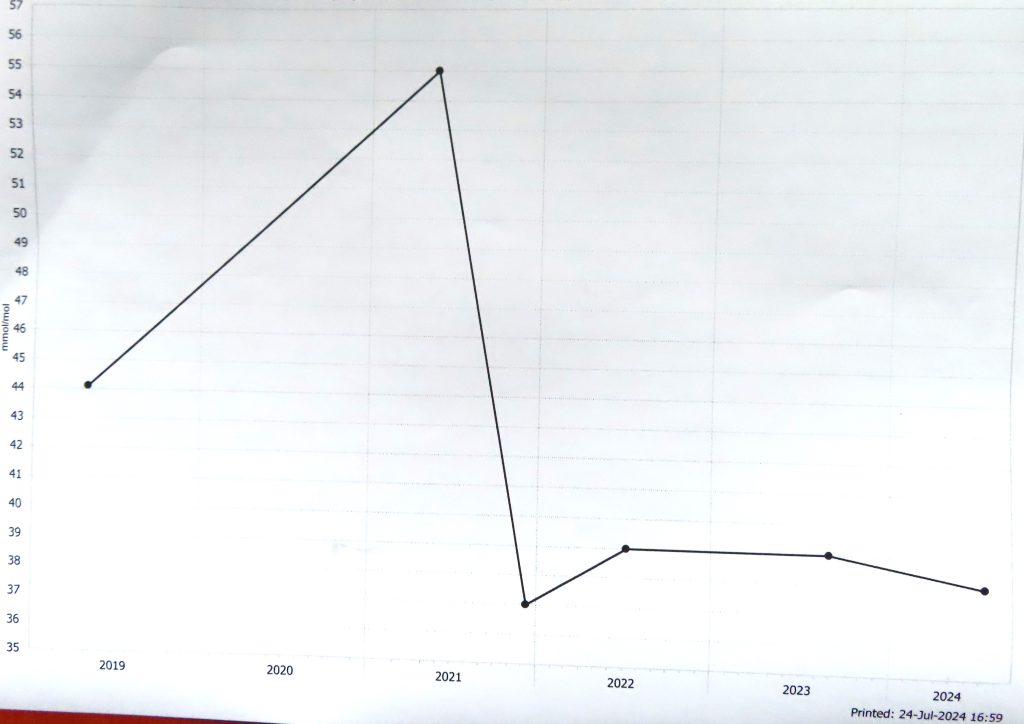
Lipids at 3/4 remission
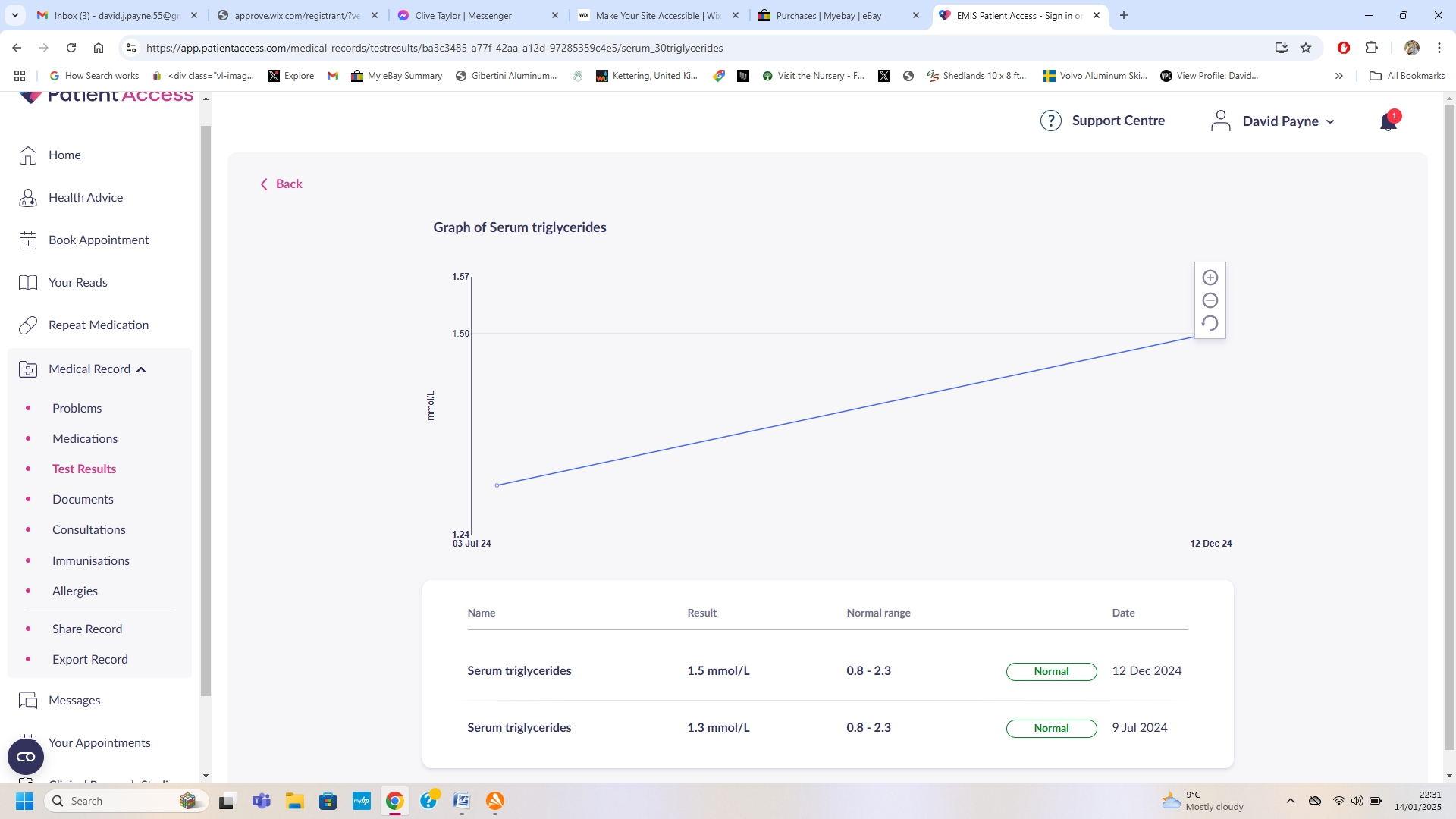
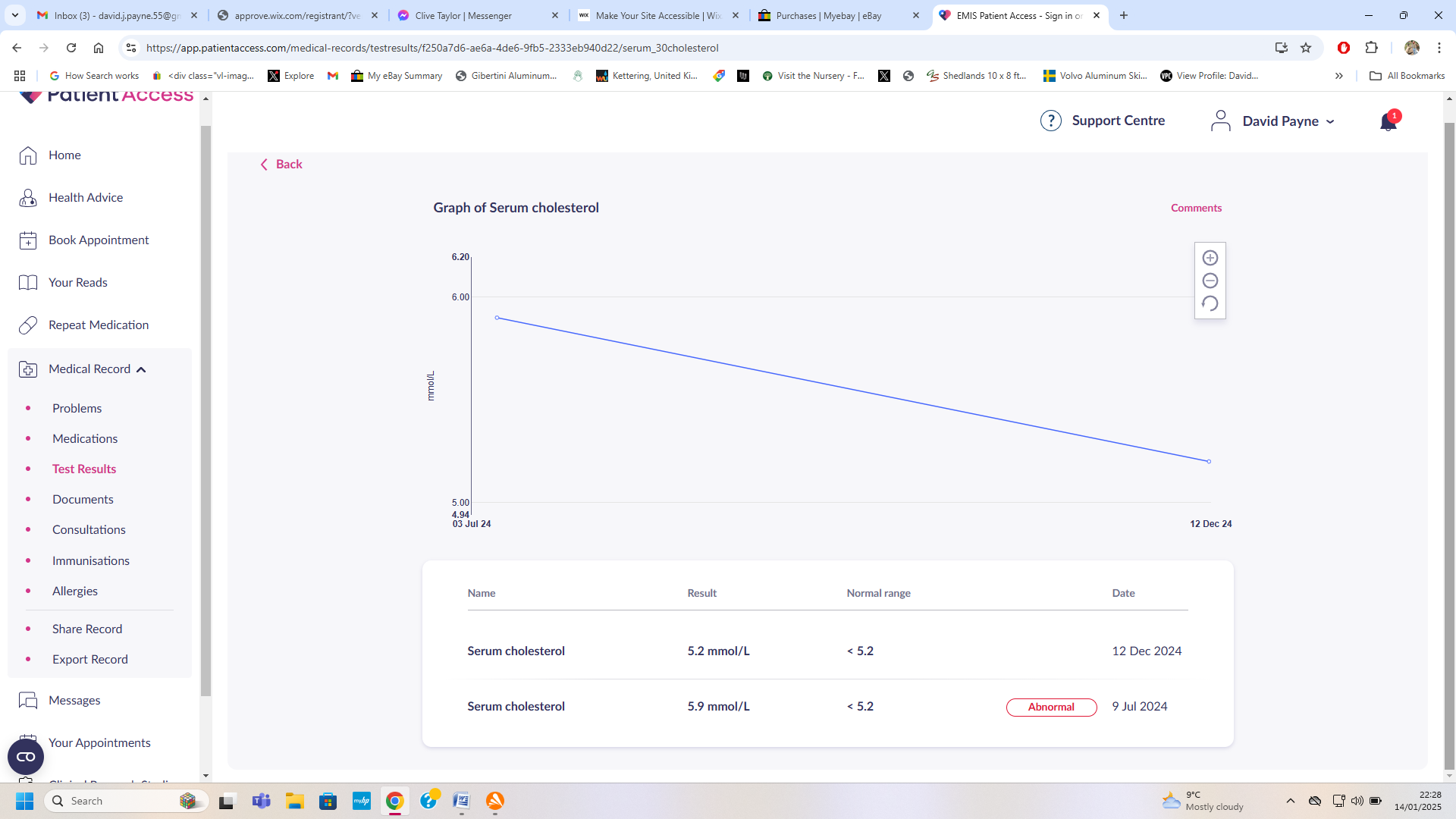
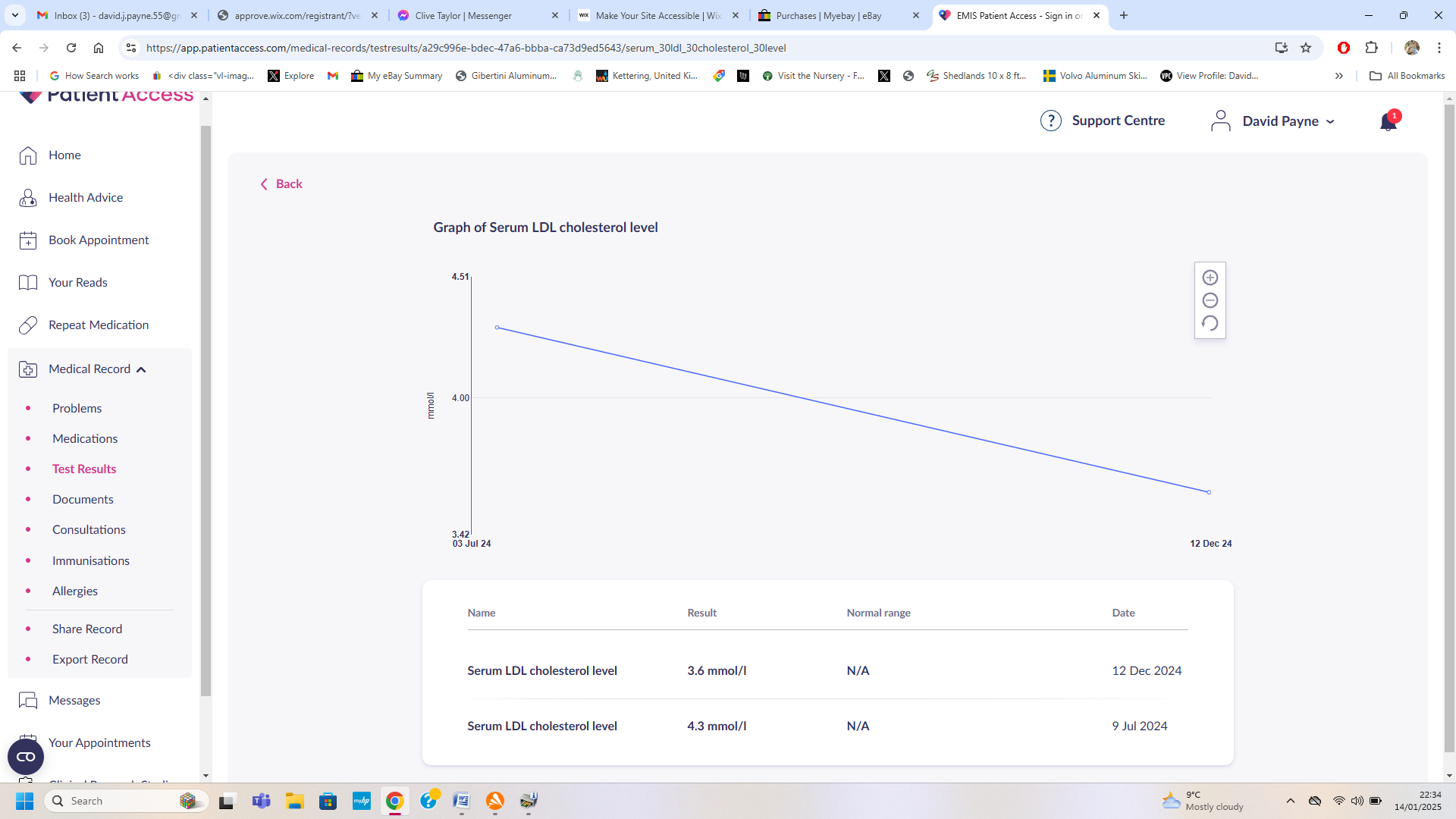
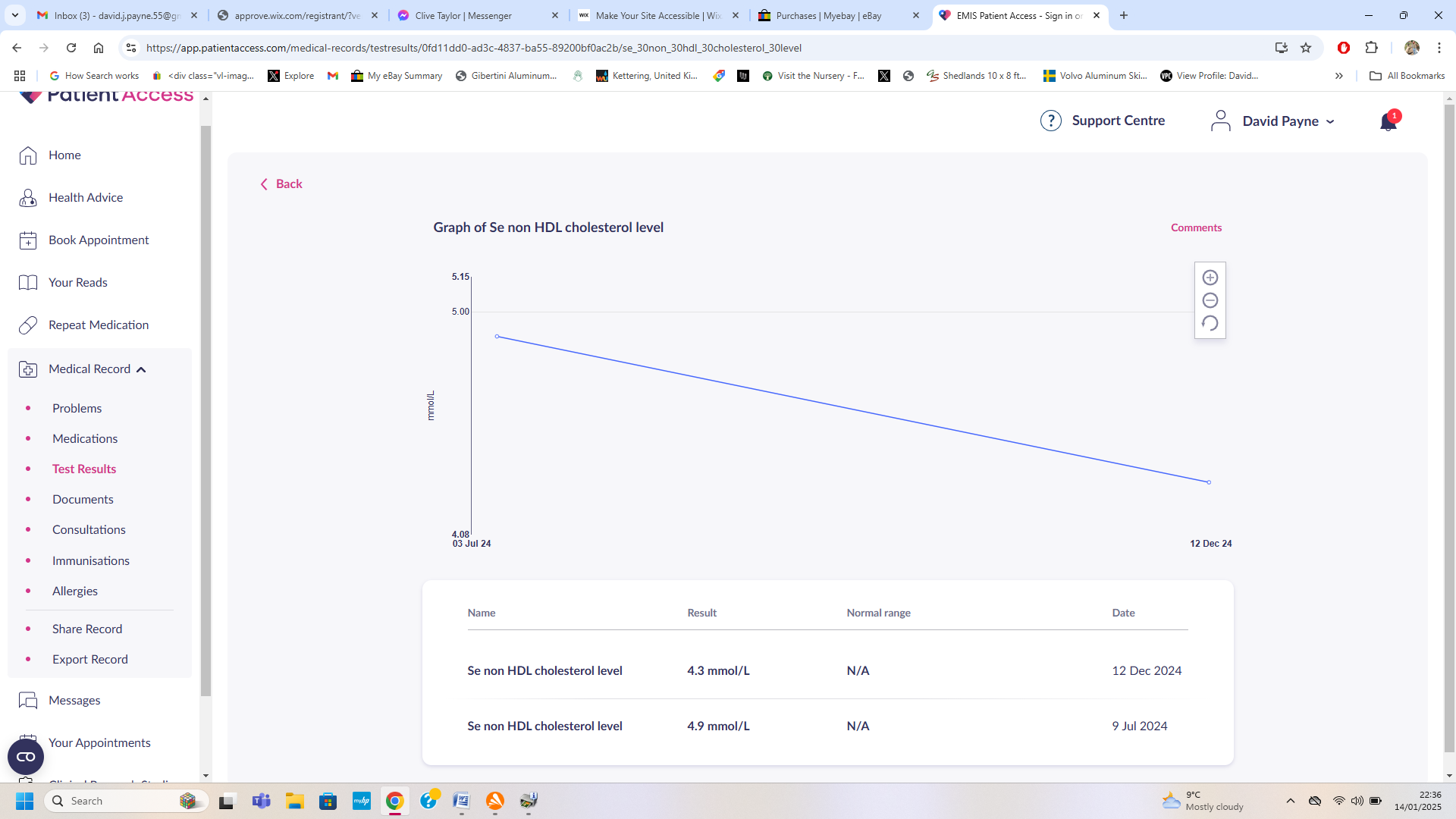
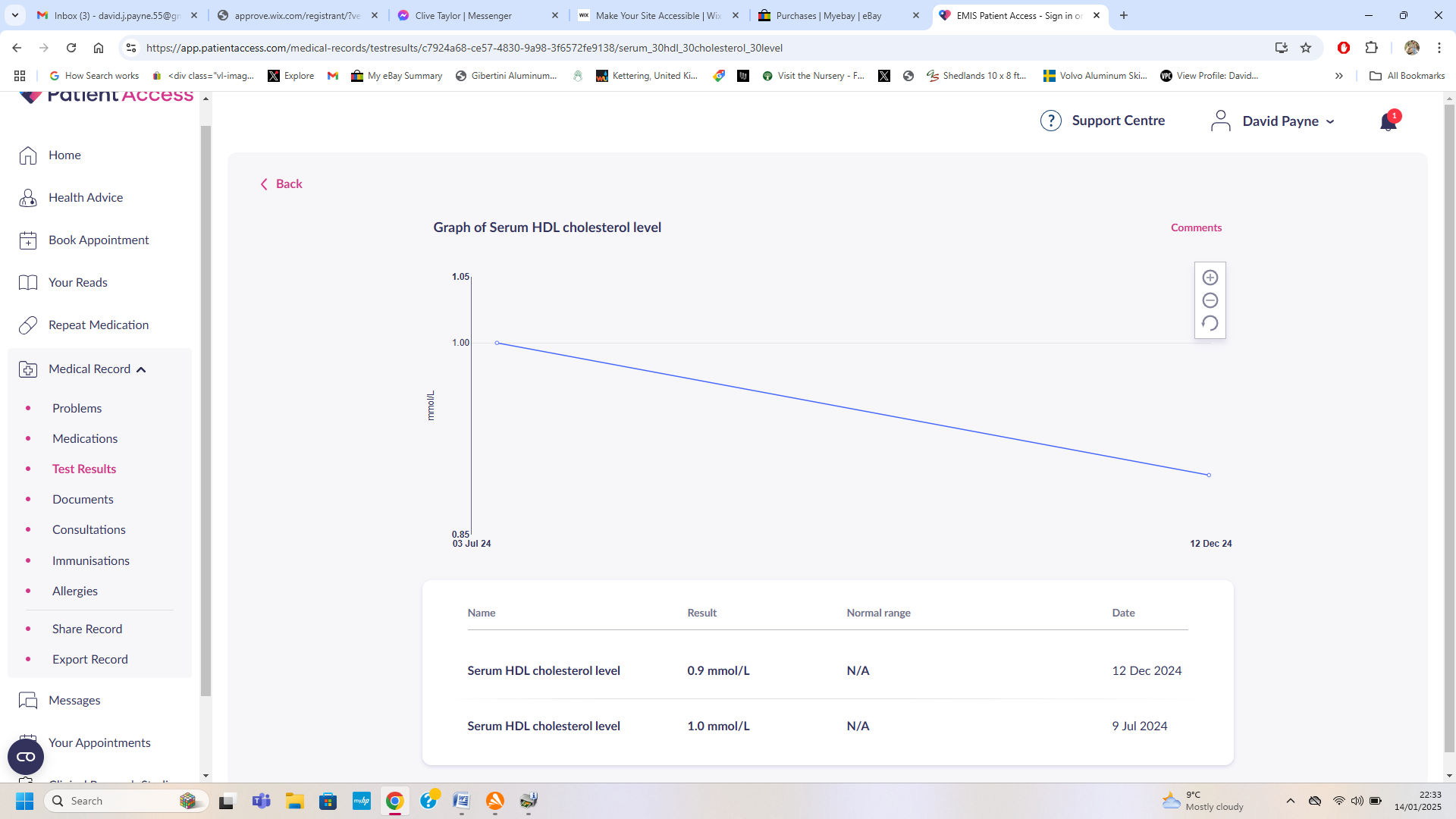


Unimaginable amounts By the handful
Exfoliation: The ever increasing amount of ‘muck’ that comes out of the skin is beyond even imagination, it is as if this is coming from another dimension. For the first year, even though little result of exfoliation could be seen, the P trap in the bathroom sink would require unblocking around every few weeks. Keratinocytes exfoliated during use of bathroom products that contain Sulphates remain active and which stick to the inside of the plumbing like superglue and set to like leather. Once the micro fibres begin to rise, the keratin behaves differently and will begin to hydrate into a stiff paste. There is so much of this exfoliated that it will clog and/or destroy both soft furnishings and even carpets. I have leather seating and vinyl flooring, from which this can easily be cleaned. Normal machine washing removes this from clothing, however, I did add laundry sanitiser and a scent booster to neutralise the lingering unpleasant smell. Quadruple Green Shield stamps, right there!
Flux: This parasitosis activity results when for whatever reason, accumulations of active keratinocytes that are surrounding a microfibre have become separated from the ‘hive’ and consequently, isolated from sufficient of the errant parasitic signal that is emitted by MD. These are in a weakened state of ‘flux’; their grip has been compromised and these are unsuccessfully trying to reattach and which happens mostly during the hours of darkness.
Humidity: Since contracting MD I have become highly allergic to mildew, consequently, I run a dehumidifier and keep my home @ around 50% which is a completely condensation and mould free environment. I have no evidence whatsoever that this helped with the MD, however, without any doubt this provides a healthier and consistent environment to live in and which removed that complication from my life.
Hydrogen Sulphide: Is a Volatile Organic Compound that has unusual affects on biology which are not understood by medical science. This gas occurs naturally in sewers, manure pits, well water, oil and gas wells, and volcanoes. Because it is heavier than air, hydrogen sulphide can collect in low-lying and enclosed spaces, such as manholes, sewers, and underground telephone vaults. Its presence makes work in confined spaces potentially very dangerous. Symptoms of acute exposure include nausea, headaches, delirium, disturbed equilibrium, tremors, convulsions, and skin and eye irritation. Inhalation of high concentrations of hydrogen sulphide can produce extremely rapid unconsciousness and death. The health effects of hydrogen sulphide depend on how much H2S a person breathes and for how long. However, many effects are seen even at low concentrations. Effects range from mild, headaches or eye irritation, to very serious, unconsciousness and death.
(I suspect it’s no coincidence that errant keratinocytes floating on hemp balm have a similar metallic appearance to H2S floating on water?)
MD Components Oxygen Tolerances:
Sores; Aerotolerant anaerobes
Microfibres; Moderate anaerobes
Fibres; Strict anaerobes
Endospores: Aerotolerant shell with obligate anaerobes core
The human dermis is well-oxygenated, the epidermis is modestly hypoxic and portions of some sebaceous glands and hair follicles are moderately to severely hypoxic. This reveals why MD is prolific under hair.
Oxygen levels in the skin can be measured using a pulse oximeter, which clips onto a fingertip, earlobe, or toe. This device measures how much light passes through your skin, which is affected by the amount of oxygen in your tissue. This reveals why clip-on pulse detectors are unreliable on me.
Mental Health: As my revelations and recovery have undoubtedly proven, MD is not a delusional parasitosis mental health issue; nevertheless, this ailment is relentlessly ‘uncomfortable’, which over time does erode the ability for rational thought and consequent to many patients I have tried to help having an endless list of unlikely and/or irrational excuses to avoid terminating this intimate association, leads me to suspect that MD has a psychological influence to perpetuate its own existence/survival?
My personal experience of this was in three aspects; despite previous to MD presenting myself clean shaven and with a no.1 haircut, cutting any of my hair was unusually ‘challenging’. Despite previous to MD being a beer drinker, drinking sufficient liquid was another challenge. Finally, I have never before used moisturising cream; however, I found this unusually challenging too. Fortunately, I was strong enough to get the better of this, which was essential because I live alone, however, I suspect that many may not have such power of will and could require encouragement and support from their partner/family members to overcome?
It would be wrong of me to tar each & all with the same brush, my recovery is evidence that is not the case, nevertheless, I strongly suspect that MD has influence over behaviour. This entire-body encompassment appears to nurture a condition that I could liken to somewhere between Stockholm syndrome and drug addiction, which is revealed with/by defending MD’s continuing existence with denials, untruths, fabrications and/or emotional outbursts.
I am not completely unqualified to mention this; I do have a degree in Psychology and my life experiences include 20 years of teaching disadvantaged students various and also losing a close friend to Class A drug addiction. Autoimmune disorders are so fully encompassing, I am certain these are more than skin deep.
Notably, so far to date, the only person who has taken my advice seriously, turned out not to have MD at all, but alternatively, a parasitic skin infestation.
I can save people from Morgellons Disease; I can’t however, save them from themselves!
Nemesis for components:
Sores are acidophiles: nemesis is; antibiotics & bicarbonate of soda.
Keratin (ocytes) are acidophile influenced: nemesis is bicarbonate of soda & hemp balm.
Fibres anaerobes; nemesis is oxygen only.
Microfibres; are anaerobe archaea, nemesis is oxygen and/or antibiotics.
Reproductive endospores; exfoliation only, nemesis; burn them with fire.
Neosporin Original: This product I discovered late in remission, it had no noticeable effect on crystallized sores, bicarbonate of soda is the nemesis for those acidophiles, however, this product was very affective with the less concreted sores in my eyebrows and was good at encouraging out the keratinocytes. I strongly suspect that there could be great advantage from switching between different topical antibiotics to keep ‘Venom’ guessing; however, because of the ridicules I have had with doctors, it wasn’t worth risking another Green Shield stamp to find out? I strongly recommend that this tactic should be tried. I suspect this also could be beneficial with the orally taken antibiotics too,
Oxygenating skin: There are many ways to oxygenate your skin, including
Increasing circulation: Activities that increase blood flow to the skin, like exercise, a facial massage, or a hot bath, can help oxygenate your skin.
Breathing exercises: Deep breathing and pursed-lip breathing can increase the amount of oxygen in your blood.
Skincare products: Using dedicated skincare products can help oxygenate your skin.
Exfoliating: Exfoliation can help oxygenate your skin.
Dry brushing: Dry brushing can help increase circulation.
Facial massager or roller: Using a facial massager or roller can help increase circulation.
Stopping smoking: Smoking can restrict blood flow by narrowing artery walls.
Staying hydrated: Staying hydrated can help increase circulation.
Oxygen tent?
Hyperbaric chamber?
Photoreactive: Keratinocytes exfoliation is difficult to encourage during daylight without use of THC, from which far more benefit results from administering late in the evening which then exaggerates this ‘natural’ rhythm. This bizarre quality began at around 10pm and continued to increase until I gave up and went to bed. MD rarely reveals itself until dermatologists are safely tucked up in their beds. I have detailed the times that I employed in the schedule, which maximised remission without minimising necessary life duties during the daytimes. I did however; continue on later into the night during waves of productive remission at the weekends. However, you are your own physician and everybody’s life schedules are different. Notably, MD was not fooled by using blackout curtains?
Following the stress that was enforced upon me by my heinous GP, unsurprisingly, I had problems with sleeping. The consequent daytime tiredness resulted for the first time with ‘moderate’ keratinocytes exfoliation during daylight. This I suspect reveals that MD is not as religiously photoreactive as I had surmised. However, the horrendous experiences of pain endured resulting from keratin separating from nerves every night for 9 months during the experiments on myself contradicts this.
This results with me believing that both of these are factors which can combine that exposes further psychodermatological influence of this archaea infection, because when we are tired, which is generally when it’s dark, we normally go to bed!
This exposes yet another ‘tumbler’ on MD’s combination lock.
Like tumblers in a combination lock

Keratin purging around my eye
Purge: A sensation resulting from the expansion of decompressing keratinocytes that are trapped and/or partially trapped beneath sealed follicles. This is strongest in the areas of initial infection, which consequently have the most microfibres. This manifestation can be clearly seen around the eyes.
Radweld; (Extract from official description) “think of the actives as a mixture of a sticky material combined with a number of different particulate materials.
We very carefully control the level of sticky material and the size of the particulates in order to achieve a balanced binding at the site of the damage, to make sure we seal those holes that we want to seal, and ensure we don’t cause any blockages.”
Research: Much of my ‘research’ is both irrelevant and also way too abstract for comprehensible description, this obscure snippet however, is important. Most of the consequent pain and/or discomfort that I have endured whilst researching for this remedy are not worth mentioning because the succeeding program has been developed to minimise and/or avoid these. Nevertheless, for the benefit of those who may think they know better; the most active and painful parasitosis events are when keratinocytes are in a state of ‘flux’. Separated from the ‘hive’ and consequently, dithering in between a locked and unlocked state. During which time this substance can spring into like glass shards up to quarter inch long within the skin and then grip & grab at nerves trying to reattach. This felt like being stung by bullet ants whilst being eaten alive from the inside by cockroaches, in every single follicle from head to foot. At this time I had discovered elements that encouraged this activity yet not the elements that alleviated the consequence. However, I understood that MD hurt me when I hurt it and I’m a stubborn old man.
Continuing to research for ways to control keratinocytes remission in a manner which avoided this consequence, I endured this state of flux activity, every single night for at least 9 months. The pain and parasitosis became so intense, I would break into a cold sweat whilst my whole being descended into ‘white noise’ and then blipped in and out of consciousness until sunrise when the keratinocytes would regain strength, reattach and the pain and discomfort would then stop, as if by magic. The only way I found respite, was soaking in the bath. Subsequently, I discovered hemp balm and bicarbonate of soda, which when used as I have further researched and recommended, holds the keratinocytes in unlocked formation during peak remission times and which transformed this essential procedure to become what I would class as; manageable ‘mild discomfort’.
For the benefit of potential Pickers & Mixers, this eventuality would be encouraged by showering instead of bathing, or bathing without bicarbonate of soda when combined with using only 50ml of CBD cream (or maybe hemp balm?) per day. Should this mere snippet from my research not deserve a drink, I shall remain happy to never meet you in a pub!

Unimaginable amounts
Rubbing: Rubbing is an essential art; a strong pressing rub with one finger helps to break the keratinocytes crystals, best employed in the same direction as hair grows. As remission progresses, less pressure is required and more fingers can be employed. When exits are locked, the ‘flow’ backs up around the follicle like a donut. Light rubbing at the right times breaks this lock.
Scratching: Manic scratching is bad, broken skin only exacerbates the matter. However, targeted ‘nudging’ with a fingernail is sometimes essential. The keratin (ocytes) is most determined to glue & grip, right at the points of exit, where/when with/for large deposits the follicle appears to dilate and it’s possible to ‘nudge’ this without touching the skin at all. Inside ears are the most challenging places on the body and where careful ‘nudging’ will be of most benefit.
Skin: You might not think so at this time, but please don’t forget that your skin is your ‘friend’. This is constantly trying to help you by exfoliating what it can. Damaging your skin reduces its ability to do so.
Squeezing: Don’t do it! This actually drives MD in, not out and results with nothing but pain, alternatively however, stretching out the skin can cause MD to rise up. Keratin (ocytes) and the fibres when ‘ready’ will rise out gently with rubbing and eventually will raise out without assistance, however, ABSOLUTELY DEFINITELY not before.
Stress: Whilst under stress, exfoliation of keratinocytes is turned off like a tap!
Tiredness: Tiredness is an associated symptom further to the brain fog which is caused by MD. This is consequent to the immune system constantly working hard and also an all consuming lethargy of the whole body’s metabolism. I hadn’t accepted how much this had affected me until remission was almost complete, whereupon, my appetite improved, I became more physically active and the brain fog began to fade.
Peak exfoliation definitely takes place during the nights, but only if and when you are tired. Should your sleep routine be out of rhythm which results with being wide awake in the middle of the night, keratinocytes exfoliation is reticent. It appears that the more tired that you are, the more that keratinocytes can be exfoliated. Ironically, when MD is dead, the exfoliation of keratinocytes switches to happen during the daytime.
I could have earned triple Green Shield stamps for that one!
Touch screen technology: Keratinocytes in the skin interfere with the ‘usual’ operation of these devices. Sometimes it can be challenging to get these gadgets to respond, yet at other times can be too ‘frisky’ to use.

Weight loss
Weight Gain: This is an accumulation of fibres and/or micro fibres & keratinocytes. I was only moderately over weight, nevertheless, during the last few months of remission I was steadily losing weight at around half a kilo a week, which is an indicator of the immense volume that needs assistance to decompress.
Yes there really is that much of it!
Final stage remission is like an instant weight loss program, actually rising up and out of the skin. Be prepared for this last phase, the good news is; this is completely painless, the not so good news is; this is remarkably messy, everywhere you go leaves a trail.
This weight literally falls off!
Excessive weight gain resulting from inactivity and/or poor diet and/or comfort eating is an influence of MD, the more flesh that there is, especially fatty low oxygenated flesh, the more prime real-estate MD has to occupy and is a portrayal of the ever increasing control and which will require a ‘standard’ weight losing procedure.
Yoyo Factor: Bicarbonate of soda is alkaline and the creams are neutral pH. The alkaline bathing neutralises and weakens the acidophile sores and the errant acidophile influenced keratinocytes and the hemp balm then penetrates and neutralises this which then ‘breaks’ it. Keratinocytes appear to become resistant to regularly applied topical products. The ups & downs resulting from irregular bathing in the alkaline bathwater recipe negate this, which I believe to be an important factor for rarchaea emission.
……………
Listed below are the factors that have proven and/or suspected to be beneficial. The main elements in order of application are; Doxycycline, Balneum Plus, Bath Recipe, Hemp Balm, Scheduling, THC and Ambient Temperature, nevertheless, every little helps. Should you have a favourite supplement that’s not on this list, take that too, it certainly won’t do any harm and could even be something that I haven’t identified which is also marginally advantageous? This list begins with those that had lesser noticeable effect; however, MD is such a tenacious ailment, every little that can be done to defeat this is a small step in the right direction.
Please note: Picking & Mixing I guarantee will result with lessened or no remedial effect, or maybe worse!
Please also note: As obscure, inane or futile some of these basic elements may appear, these can and most probably will at times generate more remission than is tolerable. Administering this remedy is an art that must be learned which will vary during the course of remission and be different for each and every person. Remission is not a secret; MD encapsulates the nerves which will keep you informed of your progress. The art is learning what pace of remission is suitable/tolerable for you.
……………
Beneficial & Suspected Beneficial Elements:
Listing order; suspected beneficial – mildly beneficial – majorly beneficial.
Swimming in the Ocean: Should you be fortunate to live in a location where the oceans are not polluted with raw sewage as they are here, I strongly suspect that regular bathing in the sea and also the consequent exposure to sunlight could/would be of benefit?
Vitamin C: I didn’t purposely take vitamin C supplement, I do however, like to drink cans of orange juice & sparkling spring water and unsweetened cranberry juice. I don’t know if this helped, yet include this information because it’s what I did.
Magnesium: Bathing in this definitely helps a little, subsequently; I added magnesium supplement to my routine. I have no evidence to prove that this helps; I merely suspect that it could and this certainly does no harm.
Hydration: My research revealed that many MD sufferers do not drink enough. MD thrives in a dehydrated and acidic environment, so it’s basic common sense to ensure that you drink at least your recommended daily amount. I suggest more than. My favourites in most consumed order were; sparkling spring water, coffee, orange juice with sparkling spring water, unsweetened cranberry juice and tea. Keeping one or more of these next to me at all times certainly helped.
Diet: Eating a healthy balanced diet is also basic common sense, avoiding foods with sulphite preservatives is recommended for post H2S exposure and every little thing helps. Archaea are recognised to have connection with sugars & lipids, consequently, I chose a virtually no sugar, alcohol or fat diet. The only food item I found that noticeably helped were chillies that made me perspire, which became obsolete information after I had discovered about controlling the ambient temperature. Nevertheless, there is one other observation that might be worth mentioning. I am always varying my healthy diets, which ultimately transpired to an increase in the average amount of eggs that I ate per week, from around 2 or 3 to around a dozen. This was very late in remission and may have been completely coincidental; nevertheless, this corresponded with increased remission and weight loss?
Coffee: I took the antibiotic with my first mug of coffee of the day, which resulted with a noticeable ‘mini-purge’. One day, I forgot to take the antibiotic, yet still experienced the same effect. I suspect this resulted from the caffeine and if so, maybe tea could result with similar effect? (Marginally maybe, nevertheless, all these little things add up.) Please note: I do not take sugar in my beverages; I haven’t for now more than 40 years, consequently, I cannot know for sure if this factor had any influence? It is anomalous however, that an acidic beverage proved beneficial for defeating an organism that thrives in an acidic environment; maybe there could be further advantage to be gained from caffeine?
Dettol: Adding 2 x caps of this to bathwater resulted with the sores dissolving and falling off, maybe not every time, yet fall off they will and without leaving a scar, not even a mark.
Do not skimp on the bathing time or you will not beat MD.
More is better.
Dettol Soap: This is the only ‘body product’ in my bathroom, this contains sulphates.
Bizarrely, this chemical causes the keratinocytes that have been influenced by this acidophile to exfoliate in a different form; this/these remain ‘active’ and attach to the inside of the plumbing where they set like leather. I needed to use bathroom sink unblocker for the P trap every few weeks. The palms of my hands were the most heavily infected areas by microfibres, using soap may have denatured body oils; however, hands also receive the most hydration whilst applying moisturiser. I never dared to mention this to my doctor; whilst he only bothered looking at my skin twice during 10 years! Mental health problems are so much easier to diagnose, because there is no evidence that he needs to waste his time looking for.
Corsodyl Toothpaste & Mouthwash. Using these products; following several months of feelings like peach fur on my tongue, the inside of my mouth was the first place that MD cleared. This is because this/these products contain bicarbonate of soda?
Calcium: Consequent to MD I have lost 5 teeth, X-rays showed this was due to extensive bone loss around their sockets and my dentist suggested that MD could be robbing calcium from here. Subsequently, I began taking calcium supplement and did not lose any more teeth.
Epsom Salt: Half a pint of this added to bathwater definitely helps a little. I suspect it is magnesium that is the beneficial element.



































Light Exercise: Definitely helps. I’m not certain if this has to do with increased blood circulation delivering oxygen and antibiotics to MD, sweat gland activity or most likely a combination of both? I’m not suggesting that you waste your money smelling the sweaty crotches of others to the sound of pants music whilst surrounded by mirrors at a local gym, but doing a bit of gardening or DIY; seeing results from your labour is good for the soul. Especially the gardening; this activity grounds you with nature.
Omega 3: Blood tests revealed that my high-density lipoprotein (good cholesterol) was virtually nonexistent; consequently, I began taking cod liver oil capsules, which notably made no difference whatsoever to my HDL results. Subsequently, the ‘purges’ became a little more noticeable and I found that 3 x 100mg capsules per day resulted with maximum benefit. I suspect this stimulates the sweat glands?

Sunlight forces the sores to rise
Sunshine: When taking Doxycycline, avoiding skin exposure to sunlight is a requisite, nevertheless, there is great benefit to be had here. Not with the keratinocytes or microfibres, however, the sores don’t like this at all. Unfortunately, my home is open plan and I don’t have a garden where I can expose my body to sunlight without risking arrest and further Green Shield stamps, which has restricted me to only being able to expose my head and arms. It only took around an hour or so of springtime sunshine to cause all of the covert sores in these areas to break out, except for on the tip of my nose, which eventually revealed to be a beast. Once broken, these then continued to rise up & out and completely cleared up within a couple of weeks. I can’t objectively suggest a sunshine ‘ration’, just be sensible about it. I suspect that benefit could be had from the use of a sunlamp; I never had the opportunity to find out. However, I believe this could only provide benefit when used in the daytime, use after dark would interfere with the natural biorhythms at work here. I suggest that doing some gardening in shorts with your shirt off would be the most sensible option. (This is a major element.)
For convenience of the astute and/or inevitably those who will be hunting for reasons to ridicule and/or deny themselves and others this remedy; the sores are susceptible to direct sunlight, because these are an infection. The keratinocytes however, are susceptible during the hours of darkness because these are products of the immune system, which apparently, are weaker in the absence of daylight. This exposes the infection is weakest during daylight and keratinocytes are weakest during darkness, MD has a Yin & Yang, which both have an Achilles heel. The art is coordinating these weaknesses with other easily usable/manageable biorhythmic remission peaks. These elements function like the correct sequence for a combination lock.

Balneum Plus Cream: MD thrives in denatured skin; consequently, I avoided products that emulsified body oils. I bathed with this instead of soap. It’s the 5% urea that is the active content, this hydrates and evacuates any keratin (ocytes) that have ‘broken’ and it also helps to lift out any crystallized sores that are losing their grip.
Bicarbonate of Soda: By chance, I discovered that after I had been mixing concrete for a garden project, the small amount of cement dust that settled on my skin resulted with keratin (ocytes) rising. Deducing this to result from the lime content, yet not wishing to dust myself with cement, I knocked up a mix of; 40mg CBD cream + 10mg of Eucerin 10% urea + a teaspoon of bicarbonate of soda and slapped this all over. GOOD GOD! The resulting unexpected purge, right from the ‘roots’ was WAAAY beyond my ability to cope. Alternatively, I found that adding 2 pints of this to bathwater gently weakens the keratin (ocytes) from the top down and is not uncomfortable at all. This does contribute to the ‘yoyo’ factor of remission dependent on pH level in the skin; however, I found that daily bathing was counterproductive. Most definitely helps. (This is a major element.) I strongly suspect there is further advantage to be gained from yet un-trialled applications of bicarbonate of soda, nevertheless, I had recently endured 9 months of pain beyond description and chose to be content with the ‘comfortable’ route I had discovered. Nevertheless, I found that lightly dusting this onto skin before application of hemp balm results with a ‘seismic’ response from the keratin (ocytes). I recommend that you do not try this until late in remission, after MD has lost the ability to keep the follicles sealed.
You have been warned!
Ambient Air Temperature: I found that when the ambient temperature was below 21.5C no keratin (ocytes) were exfoliated and yet uncomfortably too much when the temperature was above 25C. I suspect these numbers could be different for others dependent on when follicles begin to perspire? By means of central heating and air-con, I endeavoured to hold the temperature inside my home at around 23C, which I found tolerable and consequently, the most consistently ‘productive’. With a temperature of no more than 20C during bedtimes to allow peaceful sleep. However, we are all different, whatever temperature equates to ‘clammy skin’ for you, is probably the best temperature for exfoliation? This remission ‘activity’, literally has an On & Off and/or adjustable switch. This most probably explains why MD is the least troublesome on/in armpits? (This is a major element.)





Monitor your winning
Bathing: Bathing is the perfect opportunity to respond to this skin disorder and there is a lot of benefit to be gained, MD thrives in a dehydrated acidic environment that no doubt is generating for itself. Bathing is an essential element which counteracts this activity and which for best results must be conducted efficiently. Cream up all over with Balneum Plus, add 2 pints of bicarbonate of soda and half a pint of Epsom salts (I don’t understand how the Epsom Salt helps, but it does, I suspect it’s the magnesium?) and 2 caps of Dettol to bathwater, get in and just lay there for 15-20 minutes. This is the perfect opportunity to be blathered in moisturising cream without making a mess. Using hands only, rub off the cream in the water and parts of any weakened MD will rise out. Then chill out and continue to soak for no less than an hour. This allows time for the alkaline water to permeate into the skin and raise the pH which weakens the keratin (ocytes). You’ll know when you have soaked for long enough, because sores will turn green, shrivel up and fall off. Rub body all over a few times before getting out. Drain the water from the bath slowly and you will see most of what MD has come out. There is always some and sometimes much; seeing this result is good for the soul. Don’t rub dry with a towel, just dab off the drips and allow the alkaline solution to evaporate dry, this leaves more of it on the skin. Allow skin to become completely dry for several hours before then generously applying the Hemp Balm. Any soaked off sores will rise again to replace with another, which will then get nailed during the next bath, this will repeat until there is nothing left in the pocket remaining to rise. The bath is your best friend; bathing is an essential part of the cure and will also give respite when irritation is at its worst. Bathing also increases blood flow, which oxygenates the skin and assists the antibiotics better access to this infection and gets the fibres worried? I found that bathing every other day was the best compromise between comfortable exfoliation and discomfort. E.g. Day of bath; moderate keratinocytes exfoliation with no discomfort, day 2; maximum exfoliation with no discomfort, Day 3 exfoliation between moderate and maximum, yet with mild discomfort, Day 4, moderate exfoliation with increased discomfort. Bathing every other day is without doubt the best compromise, however, a little variation to this routine appears to help prevent the keratinocytes from becoming resistant. Note: During final stage remission when the keratinocytes have been sufficiently weakened by the alkaline bathing, at this time may be helped along by extending bathing to every third day without consequent discomfort. (You are your own physician, do what proves to work best and don’t keep this a secret from others.)
Scheduling: MD is photo reactive and remission comes along in waves. I found that peak remission of keratinocytes and ultimately, the microfibres beneath could not be achieved until after 22.00, which then continued until daylight returned. The art is to time the remedial ingredients for their maximum effect to coincide with this most productive period. Never underestimate the benefit this makes and note that you can’t fool MD to think that’s night time with use of blackout curtains!





Sore losing Balm congealing Balm congealing Results with Results with
Hemp Balm: The more often you apply this, the more that you use and the more that you rub, the sooner you will beat MD. In the beginning, the keratinocytes will take defensive form in the skin becoming like a sheet of glass and consequently, this cream won’t penetrate. What it is doing however, is constantly neutralising the bio film on the surface, which the errant keratinocytes persevere to replace at their loss and which subsequently ‘die’ and float away on the balm. The more advanced remission becomes, the ‘furrier’ the keratinocytes become and the more of this will soak in, resulting with more of them being flushed out. This is a prime weapon.
It is not possible to use too much of this product, nevertheless, efficient application will maximise results. Creaming during the daytime, and/or when ambient temperature was below 21.5C is a holding and/or priming activity for which light amounts will suffice. Conversely however, when the temperature is up to and/or over 23C and/or after 22.00 and/or after bathing and/or whilst administering THC, lay this on heavily, wait until rubbing ‘drags’ a little and then rub and rub and rub. When skin begins to dry out and/or exfoliation begins to slow down lay this cream on heavily again and repeat. The more keratin (ocytes) that are exfoliating, the more of this will be required. In the beginning one 150ml pot per day should be sufficient, gradually increasing to 2 or 3 pots per day as & when remission ramps up and the keratin (ocytes) are hydrating, these will then soak this up like a sponge.
Keratinocytes un-sticking and detaching from nerves is ‘not-pleasant’ and MD can regain lost ground whilst you’re sleeping if you’re not moisturising enough and can/will re attach.
Whatever you do, DO NOT under any circumstances attempt to post a review of this product that mentions remedial qualities for Morgellons Disease, which wouldn’t be published anyway. I learned this the hard way, I gave such a review for the CBD moisturiser I was originally using, which resulted with me receiving an email informing me that it would not be published because this was in contravention of their trading licence. Subsequently, this product was taken out of production. The silver lining to this cloud however, lead to me discovering Hemp Balm which functions just as well if not better @ around 1/15th of the price.
For the sake of others, I would hate the same innocent and unsuspected fate to fall for this product. It appears that the Big Pharmaceutical companies which have never discovered a single cure for any disease since they have been in existence, have so much money, power and influence that it’s illegal for any other company to reveal that they make a product which might help to cure something! This however, is legally permissible as long as they don’t tell anyone!

Keratin Purging: THC in blood ‘pushes’ microfibres towards the surface to escape it
THC: Consequent to finding benefit from using CBD, I was curious to learn if benefit could also be had from the use of THC. I wanted to try adding THC oil to the CBD cream; however, here in the UK it’s not that kind of shopping and which influenced the most convenient discreet availability to be heads of the cannabis plant. I previously had smoked tobacco for many years, packing this up around 6 years ago and was myself pensive about this, not for the THC, but the nicotine habit. However, for the sake of medical research, I forgave myself for a trial effort then rolled up and smoked a joint.
WOW!
There was almost immediate positive effect, before I had even finished smoking it, the keratin (ocytes) was/were purging up and/or out of my skin. This definitely supercharges the speed and/or ‘force’ of the decompression of keratin (ocytes) for an hour or two. At peak, the keratin (ocytes) sometimes literally sprayed out of my skin. Yet only @ around two or three evenings per week, regular use resulted with lessening of effect. CBD is recognised for having ‘normalising’ properties, smoking cannabis whilst moisturising with CBD/hemp cream/balm, somehow works as a THC catalyst that supercharges the CBD effect in the skin?
The first joint smoked after at least 4 days of abstinence nurtures the greatest response. I found maximum effect from smoking 2 of these on 3 evenings per week as detailed in the schedule. A little less benefit is experienced on the second day and noticeably less the on the third. The 4 x day abstinence is absolutely vital to reset/recharge this positive remedial reaction. The difference this obscure element makes to remission is MASSIVE. This response can initially be ‘uncomfortable’ as the rising keratin (ocytes) which can be clearly seen around the eyes backs-up just under the surface of the skin. Copious creaming and rubbing aids this to exfoliate. Should or when the positive remedial effect begin to wane, extend the period of abstinence and benefit from keratinocytes exfoliation will resume. As time goes on, this period of abstinence needs to become longer, regular habitual use quickly degenerates noticeable effect. Remedial effect also wanes as the MD wanes; however, this lack of purge is accompanied with the waves of keratinocytes remission joining up and becoming a constant.
Whatever, however it is doing this, this absolutely definitely helps, so I didn’t try and fix what wasn’t broken or challenge myself further to wonder why? I had quite enough to wonder about solving the mysteries of MD, without becoming sidetracked by the mysteries of cannabis. Administered efficiently in conjunction with the Hemp Balm is a Silver Bullet. THC works best when used infrequently, when consequently, the positive result is so pronounced there can be no doubt whatsoever. Full details provided in my recommended program. Whilst administering THC, the more often you moisturise with the Hemp Balm and the more that you rub the better.
I may as well address the predictable knee-jerk reactions here.
I am not one of the ‘find an excuse to legalise cannabis fraternity’ and this did not help at all with my back pains or arthritis, nevertheless, when used in conjunction with the hemp balm, this absolutely definitely undeniably helps. I did try making ‘space cookies’, however, this had no remedial or recreational effect whatsoever. I wasn’t able to access THC in other forms to try because of the ‘rules’ here in the UK. If the rules are different where you live, THC may be readily available in various different forms that could be tried?
Peak remission occurs at peak ‘recreation’, fortunately, my constitution is strong and I’m a sober drunk who could keep my faculties together for the copious amount of creaming and rubbing which is necessary for maximum remedial effect. Consequently, this recreational influence did not distract me from the creaming and rubbing that is essential for this to be of maximum benefit, which may prove ‘challenging’ for some if not many?
“Is this element of the remedy absolutely necessary?”
I can’t objectively answer this; however, exfoliation of keratinocytes were/was happening using CBD/hemp creams before I discovered THC, yet at a much slower pace, so my answer is; “possibly not?”, nevertheless, I can objectively add, if so, remission would take much longer? (This is a major element.)
Which begs the question: “Why would anyone not want a proven cure for Morgellons Disease?”
Please note: When the fibres begin to rise, the ‘purge’ becomes less noticeable. This is not to be misinterpreted as THC having less effect. What’s actually happening is; MD is losing the ability to keep follicles sealed, remission is not slowing down, but discreetly speeding up without the noticeable ‘backpressure’. Finally, once remission had concluded, I had no issue whatsoever with stopping smoking again. No addiction to the THC whatsoever and this intermittent use involved plenty of practice at packing up smoking; every week.
This ‘silver bullet’ I kept under my hat to avoid collecting a Green Shield Stamp for Psychosis.
Antibiotics: Doxycycline 200mg per day. Informed by doctors that it didn’t matter what time of day this was taken, I was administering the full dose in the mornings on an empty stomach. However, after a year of taking these, I discovered they had noticeably better effect when taken in 2 spaced out doses. (This information may shorten your remission, not a lot, but every little helps.) I strongly suspect that topically applied antibiotics could help a little applied directly to the sores. However, I was never allowed the opportunity to find out. (I believe antibiotics cause the immune system to slow down the production of the errant keratinocytes?)
Dosage; prior to discovering further beneficial elements, I had been taking doxycycline for 18 months @ 100mg per day and many sores had been exfoliated, however, remission appeared to be stalling. Consequently, at my last 6-monthly dermatology review that I waited more than a year for, which at this juncture was 23-months ago, I managed to cajole a prescription for 200mg per day. Should I have been administering this program from the onset, I suspect that 100mg per day could have been sufficient?
I had no side effects with/from this medication other than a mild reflux if I took the 200mg in one go with a mug of coffee on an empty stomach, despite having a sliding hiatus hernia and have had worse reactions than this from eating a pickled egg. We are all different; do whatever works for you.
Positive Mental Attitude: The most essential element of this remedy is a PMA and that ingredient is up to you. Stick to this regime as best you can and with 100% certainty, I faithfully promise that you WILL cure yourself of Morgellons Disease. If I was selling this cure it would have a money back guarantee; alternatively however, I have given this away; please don’t spite yourself by looking this gift horse in the mouth.
……………
Art of Remission:
This is an equation is between; increased sensations of parasitosis balanced with the knowledge of what is actually going on. Grasping an understanding of what these things are that you are feeling, will remove their mystery and negate consequent concerns. I have endeavoured to inform you of the causes for these bizarre and previously unexplainable happenings as accurately as I can. Forewarned is forearmed and this; ‘what to expect and when to expect it’ information will be of more help than you could imagine when their time comes and there’s an awful lot of ‘things’ going on!
I have been banging on about; learning how to understand the getting-better feelings, you being your own physician and that remission is an abstract art that must be learned.
I solved the mystery of Morgellons disease and now know things that you never knew that you needed to know, which I’m trying very hard to share from somewhere least expected. This is not a Psychotic Fairy Tale or an Internet Scam and it’s certainly not April 1st.
This is a Manual for how to cure Morgellons Disease!
Being the first and only Test Pilot for this cure with only faith in my own developing conclusions for my guide, I ran this Morgellons Gauntlet blind, barefoot and solo, finding the right way the hard way. My Rite of Passage has been EARNED and I am cured. Being the only person to Master this tenacious ailment affords me a unique viewpoint which I am trying to share. This is not an easy ride and is a great personal challenge in many ways!
Essential elements include;
Positive Mental Attitude
Strength of character
Determination, patience and inexhaustible tenacity
These crucial components are entirely your own responsibility!
This cure is DIY and there will be no shortage of consequent corroborating evidence, bigots, sceptics and those weak of will will rue the day.
With advantage of foresight, subsequent followers are forearmed with this knowledge and it is now the turn of others to run this Morgellons Gauntlet.
I don’t claim this to be the best ever remedy; nevertheless, it is undisputable that I have identified the first. There will always be more details that could be added, nevertheless, I have given more than sufficient guidance as best I can for you to beat MD.
The more people who participate, the more will be learned and the more this is shared the sooner these participants will be cured.
You now know;
What to do
Why to do
How to do
What not to
When to do
How to prime
How to start
What to expect?
When to expect
How to hold
How to control
How to encourage
How to supercharge
How to manage
How to ease
How to cope
How to stop
What could go wrong?
What more information could you possibly need?
Remission is an equation of equations which are under your control.
Learning this well, allows/develops into a somewhat “Dr Jekyll turns into Mr Hyde when the sun goes down” type of existence. Nevertheless, this does allow you to get on with your life in the daytimes and to get on with your remission during in the evenings and/or can even be turned off for short holidays without ‘losing ground’; the antibiotics will still be fielding their wicket. Every evening spent in remission is one step nearer the end of this journey. The more keratinocytes that are decompressed, the closer you are to being cured.
My starting point with this remedy was; I had endured MD for 7 years with virtually no medication, followed by 18 months taking Doxycycline @ 100mg per day whilst unsuccessfully experimenting with many different emollients, some of the sores had already risen out, yet virtually no keratin (ocytes) and none of the hairs or microfibres. Everyone’s starting point will be different and I am well aware that many are more infected than I was.
Remission goes through many different ‘phases’ which I will explain as best I can. I have purposely left their schedule ‘loose’ because this will not be a constant. The longer duration infected/affected, especially so in the absence of antibiotics, the more compressed the keratin will have become and the more fibres and sores will have accumulated, consequently, a longer duration for this greater mass to decompress is a natural expectation. Excessive weight gain will without doubt complicate remission; however, this is another factor that is entirely up to you.
Morgellons Disease manifests in varied guises, some patients have more and/or more impressive hairs and/or fibres than others whilst others have more ‘keratin’, however, both of these elements are always present. We are all different, I suspect that MD comes in different strengths and we have all had MD for differing lengths of time, the longer that is, the more infection there is likely to be and the more concentrated the keratin(ocytes) will/may have become.
The more often you apply the hemp balm and the more you rub, the faster remission will be.
The less often you apply hemp balm and the less often you rub, the slower remission will be. If/when irritation becomes too uncomfortable, focus on fewer parts of your body or/and reduce the ambient air temperature and/or ease up on the Hemp Balm and/or THC. If all else fails, have a bonus soak in the bath.
When/whilst the keratin (ocytes) is/are initially separating from the nerves, DO NOT skimp with the Hemp Balm as this will allow it to reattach, subsequently, any consequent pain will then have to be endured again.
Should effect from the THC wane, skip this for a week, later during remission maybe two weeks abstinence or more will be required and then positive evacuating effect will resume. When the THC eventually stops having an exfoliating effect you are almost cured and can drop this element from the schedule.
Nighttimes, raising alkaline pH of skin, ambient temperature over 23C, hemp balm and irregular THC each triggers keratin (ocytes) expulsion. Learn to recognise these factors and capitalise upon them by co-ordinating the resulting biorhythms. You would be forgiven for believing that the exfoliation of keratin (ocytes) will never end, however, every small amount that is evacuated is a step in the right direction that results with the mechanical grip of Morgellons Disease becoming progressively weaker.
You are your own physician and remission is an ‘art’ that must be learned, you MUST be ‘serious’ about getting better to beat this.
……………
You are now around halfway through a 35K word document and it’s time for a break.
I would like to take this opportunity to remind you what I said on the first page.
This cure is NOT a free ride and I don’t suspect that medical science will/could stump up a free ride either that could/would be in time to be of any use to you.
If they ever do?
To beat Morgellons Disease you MUST have a POSITIVE MENTAL ATTITUDE!
This is a subject not taught at school, this is a lesson of life.
I’m not going to nag, yet will demonstrate by example.
Below is a random album of just some of my PMA.
I will however, remind you that further to the MD that I have just beaten, I am a 69 years old man who lives alone. An Old Fart with degenerative spine disease, presently, 9 prolapsed discs, 6 pinched nerves, arthritis in every joint, a sliding hiatus hernia and poor eyesight. I don’t go at it like a bull in a China shop; I choose the times when my spine is calm and the weather is clement and just keep chipping away at it. I’m presently 56 tonnes into an 80 tonne groundwork project and 25 of those tonnes were dug by me on my knees like an Archaeologist, one bag at a time. If I can do this, so can you.
I’ll let you work it out?


























……………
Four differing daily routines delivered over seven days, which are timed for your efforts to coordinate with and to maximise upon photo reactive dictated peak remission. This is an ideal scenario/guide, scheduled as best I can to fit into persons ‘regular’ weekly lives, however, we are all different and this may remain impractical to regiment your life into, nevertheless, the closer you can align with this, the better.
Now it’s your turn!
Recommended Program:
Four differing daily routines delivered over seven days, which are timed for your efforts to coordinate with and to maximise upon photo reactive dictated peak remission. This is an ideal scenario/guide, scheduled as best I can to fit into persons ‘regular’ weekly lives, however, we are all different and this may remain impractical to regiment your life into, nevertheless, the closer you can align with this, the better.
Yes this is a task, yes it is a lot of work, yes it is often uncomfortable and yes it is sometimes painful. Expecting anything less from Morgellons Disease, is merely wishful thinking and yes this remedy is slow; however, that is a blessing and not a curse and despite wanting to get better, there will be occasions when you chose to slow this down. Stick at this as best you can and I promise that remission is sure, the more effort you that put in the sooner that will be, the less effort you put in, the longer this will take, getting better is not a race. The ’art’ is to get the keratin (ocytes) moving and then to keep it/them moving at a pace that you can manage. The faster it ‘moves’ the more uncomfortable it can be and everyone’s tolerance for this discomfort will be different. It’s the areas with the most keratin (ocytes) that are the most tenacious as the sores and microfibres inside have the most protection/defence from the antibiotics. The fibres will not die and rise out until the keratinocytes are almost gone. The measure of MD’s altering strength can be gauged by the power of its grip at points of exit.
Habitual cannabis users; please note that with daily use, the remedial effect wanes to virtually zero, the scheduled abbreviations are essential to maximise its effect.
This application of THC is medicinal not recreational.
Monday:
09.00: Doxycycline taken with a mug of coffee and apply Nivea Hemp Balm all over.
12.00: Take calcium, magnesium and 3 x cod liver oil capsules and generously apply Nivea Hemp Balm all over.
17.00: Generously apply Nivea Hemp Balm all over.
19.00: Generously apply Balneum Plus all over, lay in bath for around 20 minutes, rub off using hands only and then soak for at least an hour in bathwater that includes; ½ pint Epsom salts, 2 x pints bicarbonate of soda and 2 x caps of Dettol. Do not rinse with clean water, lightly dab with towel and then allow skin to evaporate dry. When completely dry, generously apply Hemp Balm.
21.00: Doxycycline. With ambient temperature at least 23C; generously apply Nivea Hemp Balm all over and rub.
22.00: Generously apply Nivea Hemp Balm all over and rub.
23.00: Generously apply Nivea Hemp Balm all over and rub.
00.00: Generously apply Nivea Hemp Balm all over and rub.
Tuesday:
09.00: Doxycycline taken with a mug of coffee and apply Nivea Hemp Balm all over.
12.00: Take calcium, magnesium and 3 x cod liver oil capsules and generously apply Nivea Hemp Balm all over.
17.00: Generously apply Nivea Hemp Balm all over.
21.00: Doxycycline. With ambient temperature at least 23C; generously apply Nivea Hemp Balm all over and rub.
22.00: Generously apply Nivea Hemp Balm all over and rub.
23.00: Generously apply Nivea Hemp Balm all over and rub.
00.00: Generously apply Nivea Hemp Balm all over and rub.
Wednesday:
09.00: Doxycycline taken with a mug of coffee and apply Nivea Hemp Balm all over.
12.00: Take calcium, magnesium and 3 x cod liver oil capsules and generously apply Nivea Hemp Balm all over.
17.00: Generously apply Nivea Hemp Balm all over.
19.00: Generously apply Balneum Cream Plus all over, lay in bath for around 20 minutes, rub off using hands only and then soak for at least an hour in bathwater that includes; ½ pint Epsom salts, 2 x pints bicarbonate of soda and 2 x caps of Dettol. Do not rinse with clean water, lightly dab with towel and allow skin to evaporate dry. When completely dry, generously apply Hemp Balm.
21.00: Doxycycline. With ambient temperature at least 23C, generously apply Nivea Hemp Balm all over and rub.
22.00: Generously apply Nivea Hemp Balm all over and rub.
23.00: Generously apply Nivea Hemp Balm all over and rub.
00.00: Generously apply Nivea Hemp Balm all over and rub.
Thursday:
09.00: Doxycycline taken with a mug of coffee and apply Nivea Hemp Balm all over.
12.00: Take calcium, magnesium and 3 x cod liver oil capsules and generously apply Nivea Hemp Balm all over.
17.00: Generously apply Nivea Hemp Balm all over.
21.00: Doxycycline. With ambient temperature at least 23C; generously apply Nivea Hemp Balm all over and rub.
22.00: Generously apply Nivea Hemp Balm all over and rub.
23.00: Generously apply Nivea Hemp Balm all over and rub.
00.00: Generously apply Nivea Hemp Balm all over and rub.
Friday:
09.00: Doxycycline taken with a mug of coffee and generously apply Nivea Hemp Balm all over.
12.00: Take calcium, magnesium and 3 x cod liver oil capsules and generously apply Nivea Hemp Balm all over.
17.00: Generously apply Nivea Hemp Balm all over.
19.00: Generously apply Balneum Cream Plus all over, lay in bath for around 20 minutes, rub off using hands only and then soak for at least an hour in bathwater that includes; ½ pint Epsom salts, 2 x pints bicarbonate of soda and 2 x caps of Dettol. Do not rinse with clean water, lightly dab with towel and allow the skin to evaporate dry. When completely dry, generously apply Hemp Balm.
21.00: Doxycycline. With ambient temperature at least 23C, generously apply Hemp Balm and rub.
22.00: Generously apply Hemp Balm administer THC and rub.
23.00: Generously apply Hemp Balm and rub.
00.00: Generously apply Hemp Balm administer THC and rub.
01.00: Generously apply Hemp Balm and rub.
02.00: Generously apply Hemp Balm and rub.
Saturday:
09.00: Doxycycline taken with a mug of coffee and generously apply Nivea Hemp Balm all over.
12.00: Take calcium, magnesium and 3 x cod liver oil capsules and generously apply Nivea Hemp Balm all over.
17.00: Generously apply Nivea Hemp Balm all over.
19.00: Generously apply Nivea Hemp Balm all over.
21.00: Doxycycline. With ambient temperature at least 23C, generously apply Hemp Balm and rub.
22.00: Generously apply Hemp Balm. Administer THC and rub.
23.00: Generously apply Hemp Balm and rub.
00.00: Generously apply Hemp Balm. Administer THC and rub.
01.00: Generously apply Hemp Balm and rub.
02.00: Generously apply Hemp Balm and rub.
Sunday:
09.00: Doxycycline taken with a mug of coffee and generously apply Nivea Hemp Balm all over.
12.00: Take calcium, magnesium and 3 x cod liver oil capsules and generously apply Nivea Hemp Balm all over.
17.00: Generously apply Nivea Hemp Balm all over.
19.00: Generously apply Nivea Hemp Balm all over.
21.00: Doxycycline. With ambient temperature at least 23C, generously apply Hemp Balm and rub.
22.00: Generously apply Hemp Balm. Administer THC and rub.
23.00: Generously apply Hemp Balm and rub.
00.00: Generously apply Hemp Balm. Administer THC and rub.
……………
Last year’s present from my ‘care providers’ was a 20 months delay for my 6-monthly dermatology review, presently, 23 months & 2 weeks into taking 200mg of doxycycline per day, with the remedy developed to as detailed above and it’s Christmas; which appears to be the season of bad will for ‘care providers’!
My GP, who has only looked at my skin twice during 10 years and did not respond to my written request for him to witness peak remission and despite being informed that I was well on the way to beating MD, contravened our previous agreement and complied with instruction from the senior dermatologist who 4 years ago had diagnosed delusional parasitosis and recommended cognitive behaviour therapy followed by her steering clear of examining me since that time.
Without consultation, explanation or even notification; halved my prescription for the antibiotics!
Full remission I estimate to have been a ‘few’ months away? However, with the antibiotics halved, probability of my recovery was reduced to maybe never?
My regular liver function blood tests were all A. okay, nevertheless, here we bigot go again!
I had nearly 4 weeks of pills in stock, which meant I could stretch the 200mg dosage out to almost a couple of months.
Consequent to the pain & discomfort I had endured to identify this calm and gentle remedy, I was content to continue remission like this until cured. However, with the rug pulled out from under my feet, left me with no other choice than to begin running the torture myself gauntlet again!
Determined not to fail at this last hurdle, I increased the bicarbonate of soda in the bathing recipe up to 3 pints with the half pint of Epsom salts, which was the maximum that would dissolve in my bathwater, omitted the Balneum cream, and soaked in this stronger brew for an hour. Simply rubbing my skin without using further products which can have mind bending consequences as I explain elsewhere! Following which, I left my skin dry for 12 hours before beginning to neutralise with the hemp balm. Consequent from long exposure to this caustic solution; this I was literally itching to begin, whereupon, the hemp balm congealed all over my body, something it had only done before in random here & there places. Bathing in this super caustic ‘dermatologist-scaring’ recipe, I reduced to once per week.
I hadn’t used THC for about 7 weeks because I had been content with the ‘speed’ of remission without it and smoking is bad for my health. Slow & steady wins the race; it’s a far gentler ‘ride’ too which had let me get on with writing this paper.
In for a penny, in for a pound, I added the THC back into my schedule to supercharge this supercharged remission and changed my life routine to stay up creaming and rubbing until 3 or 4 in the morning every night to maximise my efforts.
Consequently, there began ‘A Great Rising’, including on the soles of my feet where no remission had been evident before.
DON’T GET OVER EXITED; I was already well on the way to becoming cured and I can’t go back to experiment curing myself again in other ways; this now is the responsibility of others!
I did not have any adverse reaction to this stronger brew, however, I don’t recommend doing this. I am a powerfully built person and sport a hardy physiology that many if not most others won’t have; and I had no other choice.
However, this does expose that there is advantage to be gained from adjusting administration of the bicarbonate of soda.
NOBODY will believe the volume of keratin (ocytes) and fibres, which appear during this phase of remission until they have experienced this for themselves!
This/these are multi-stratified in the skin and which appear from ‘nowhere’ in slow-mo, like how bubbles appear as water boils, which then slowly inflate to become like bubble-wrap within the skin, stacked with the smallest bubbles on top, largest at the bottom with each bubble full of microscopic bubbles dedicated to an individual follicle from where these ‘decompress’ by crystallizing into ever smaller form until like miniscule hollow glass spheres that disappear without trace when they break. This continues until the bubbles have decompressed whilst the fibres within retract from the skin along with it and form into like little balls of ‘hat felt’ which when the keratin (ocytes) are depleted, then rise up and are shed from the skin!
The more that is learned about Morgellons Disease, the more unbelievable it becomes!
With no change to my diet or lifestyle, during the last 14 weeks my weight reduced by 6kg and I presently weigh in at 84kg. I was 5’ 11 3/4” before my spine began degenerating; I am now 5’ 8 1/2” and consequently have no idea how that relates to BMI?
Two weeks into this super caustic regime, I received a summons from my GP. Expecting further ridicule, I arrive armed with 9 x10” x 8” colour prints of the photographs displayed in this document and a 50ml pot full of some of debris that I had exfoliated the evening before.
It appears that ordering my antibiotics a week early to allow for delay with items posted during the Christmas period had been claimed to be ‘another’ mental health problem! Despite the ‘normal’ result from my liver function blood test and despite the undisputable evidence that I presented, he informed me that a meeting about me had been convened with doctors none who had examined me for more than 4 years, had decided that I had a mental health problem, because an incompetent senior dermatologist at the local hospital had incorrectly said so. The professor’s subsequent ‘correct’ diagnosis of Unexplained Dermopathy has been ignored and dismissed and won’t even be spoken of! He tried very hard to ignore the evidence, refused to examine my skin and announced that he would not be prescribing any more antibiotics for my mental health problem!
Even a child could see that it is not I who has a mental health problem!
I resisted his deliberate and repetitive goading and refrained from an outburst of truths about his incompetence and stupidity, because this ridicule that has been generated by incompetent ‘doctors’ with heinous power, places me one false step away from being sectioned for their insanity!
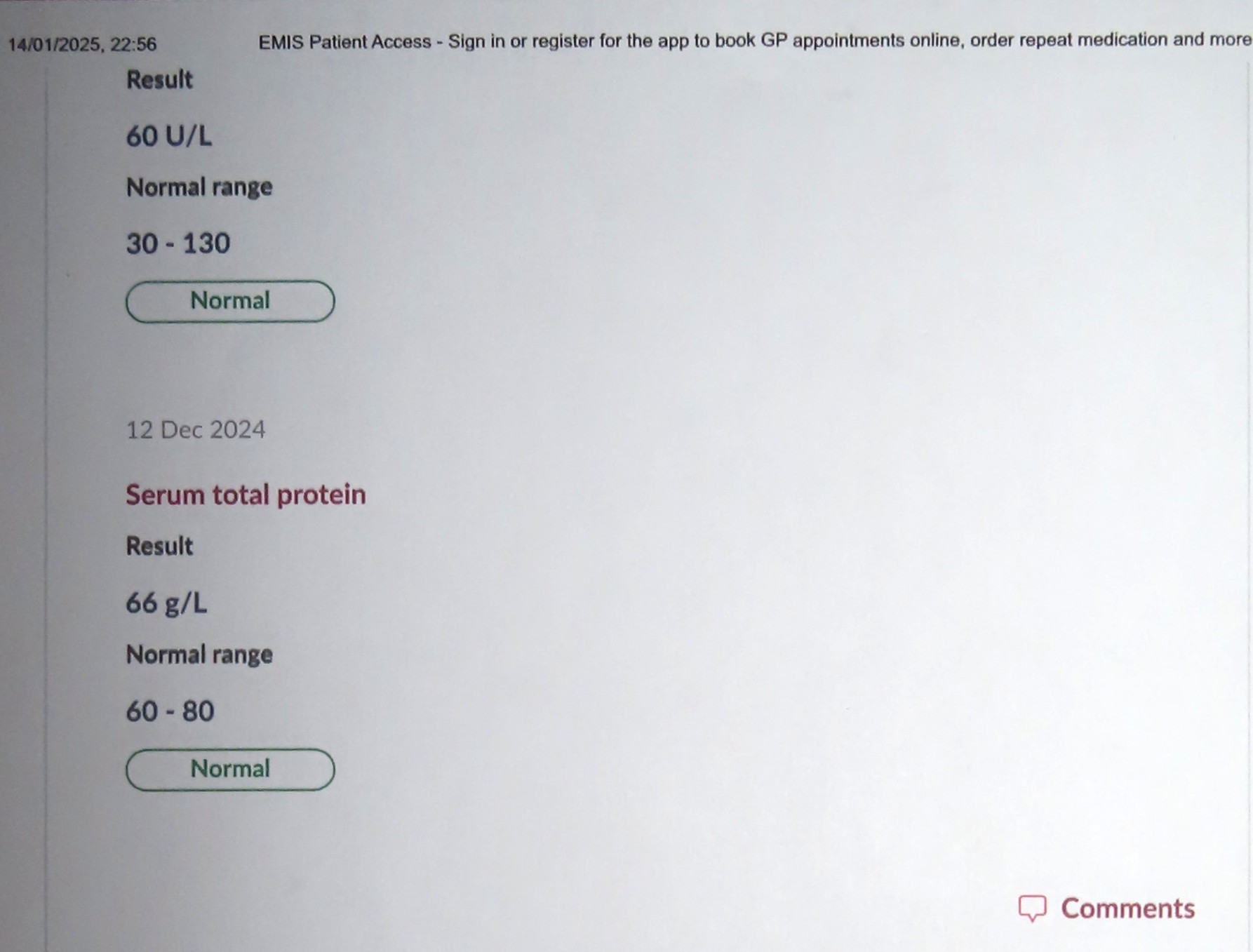
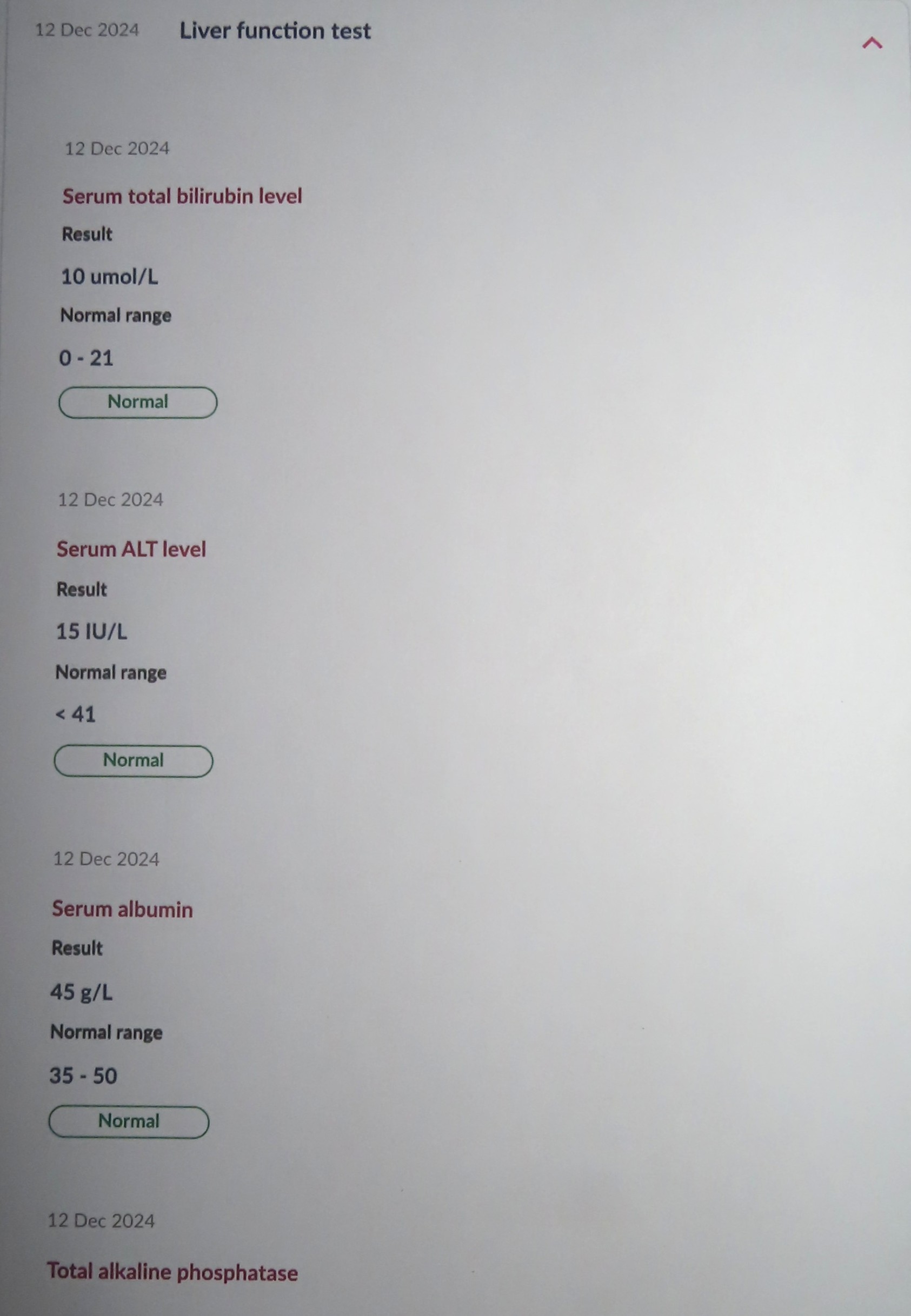
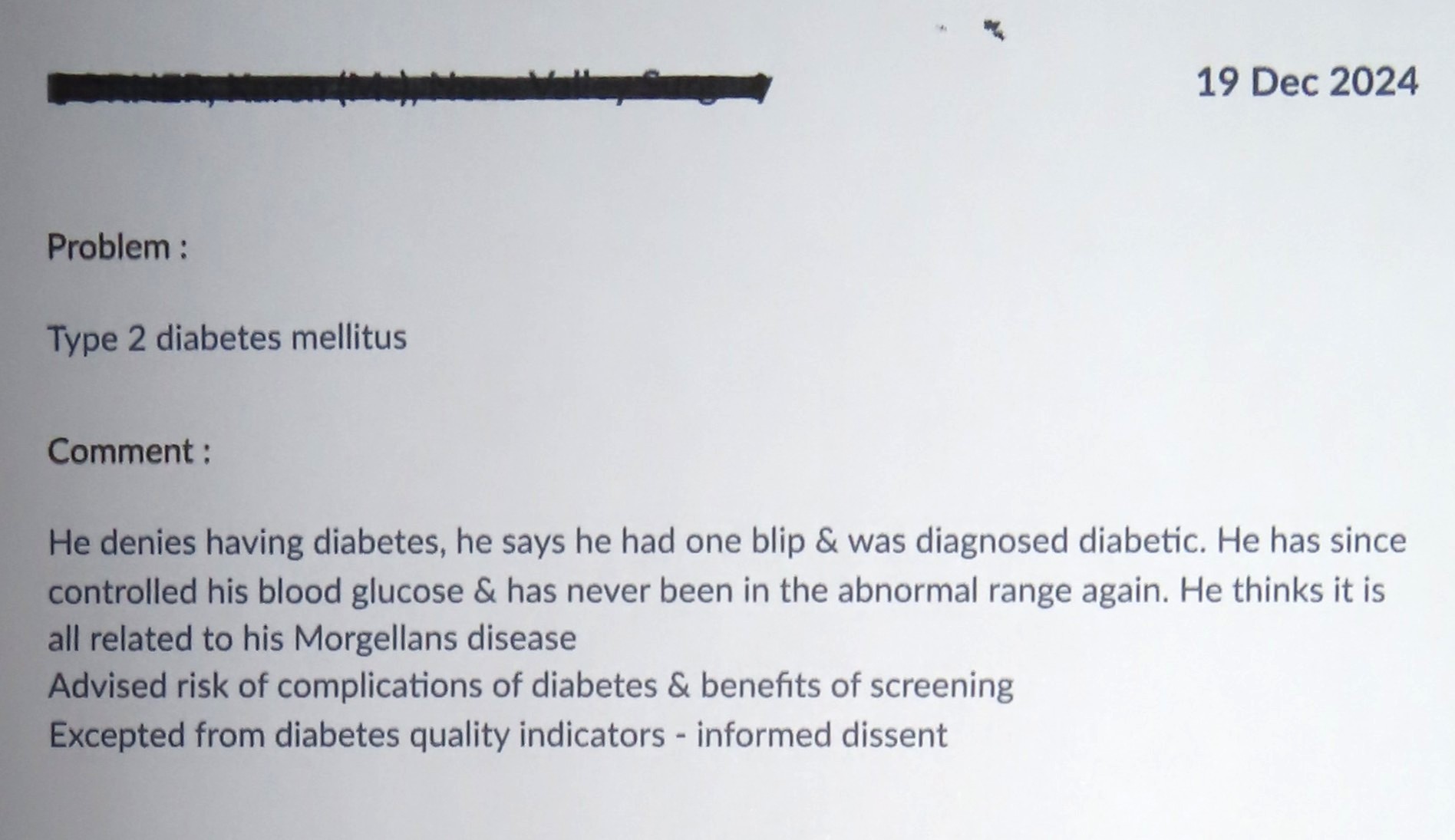
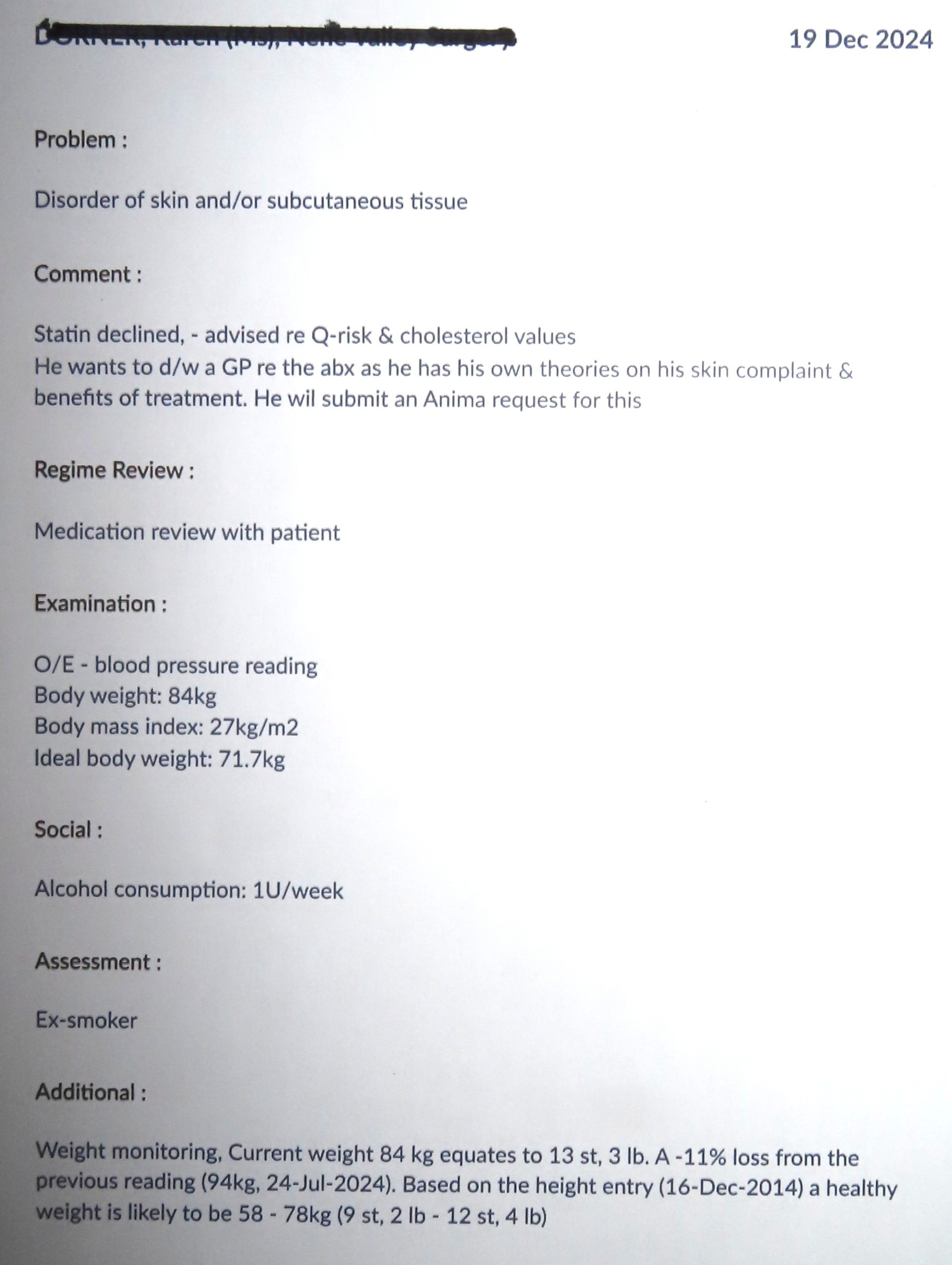
Reporting to Authorities such malicious heinous malpractice goes something like this:
“How many Green Shield stamps did you say Sir? Don’t call us, we’ll call you!”
That’s Incident number: 305 that we’ll do fuck all about this week!
It’s highly unlikely that I am the first patient that my extremely unpopular GP has taken a dislike to; this was well practiced delivery of malicious infantile revenge which I suspect could be a serial activity?
In response to a text message requesting feedback about his service, I had accused him of incompetence and nothing flushes out dishonesty more efficiently than the truth.
I have ZERO tolerance for bullies!
As if I didn’t have enough shit on my plate, this latest shit exposes that my doctor is a fucking psychopath?
Furthermore, I am beginning to wonder if I have also exposed yet another archaea infection?
The only thing that is anomalous about my mental health is that 99.99% of doctors are not astute enough to understand what I have been trying to tell them!
I can only hope that this document results with this collection of Green Shield stamps being removed from my book?
I am literally being persecuted with doctors incompetence!

Not even an official enquiry will be able to cover this up!
Meanwhile; back at the Ranch:
My options were running out and I refused to accept failure consequent to this heinous activity.
Responding to this unexpected challenge, the super caustic dermatologist scaring bath recipe I increased to every other day and I was pleasantly surprised that this caused me no consequent issues with my skin whatsoever.
To cut a long story short, this kicked MD’s arse out of my system in only a few short weeks and consequently, I beat my ‘impossible’ impossible deadline with 2 weeks to spare. Which just so happens to be the inaugural date for the new government in the US; who have appealed for unknown cures to use for/with their ‘Make America Healthy Again’ project, maybe my revelations will be appreciated there? My GP had intimated that the hospital dermatology department would not issue antibiotics to me either! So to make sure, I went to see Professor Bewley in London and literally blew his socks off with my discoveries and achievement, who was quite content to issue a prescription for the 3 months of antibiotics that I requested.
Don’t get over excited, I was well on the way to beating it anyway; however, I say again, you are your own physician. Monitor what is going on with your own body, be responsible and do whatever suits you best. Anyone and everyone will be different.
……………
Please note: The entirety of the head is the region most infected by the microfibres; here I recommend generously applying the hemp balm at least once every hour that you are awake. This should alleviate most if not all of the parasitosis and hasten comfortably the remission.
Repeat and continue until cured; when the time comes that MD ‘loses its grip’, continue with this program until ALL of the ‘debris’ has been exfoliated and then continue with this program for at least another 3 very happy months.
(Maybe there could be slight benefit from drinking coffee or possibly tea with the evening antibiotic? I never did, the ‘wave’ of evening remission was ‘sufficient’ for me.)
Remission is challenging in ‘special’ ways and I predict that the next person to beat MD will be a weekend cannabis smoker who has a loving, caring and ‘persuasive’ partner and it was she/him/it who read about this cure?
The great irony is; feeling-better is the opposite of getting-better, MD hurts you when you are hurting it, consequently, the unpleasant sensations are actually; sensations of getting better. These potions & lotions can be adjusted to best keep the keratin (ocytes) moving and rising out at a steady pace that is ‘comfortable’ and this ‘comfortable’, will vary greatly from person to person. It’s possible to work too hard at getting it moving, only to then learn the hard way that a slower and steadier pace is the better route for the nearly 4 million jammed up follicles to pursue. Morgellons Disease is photo-reactive and remission comes along in somewhat random yet increasingly often late-evening ‘waves’, in between which there can be periods when you could suspect this has stopped working.
Don’t let MD fool you into a false sense of security, stick at it.
……………
Remission:
With my own remission gradually and continually developing over the course of 2 years, my remission schedule is only loosely definable and trying to measure this against the unknown circumstances of others, timeline and duration estimates can only be futile measures. Until there exists records for numerous recoveries; what to expect and in which probable sequence is the most useful information at this time.
This is MD punishing you Don’t give in
The first thing that will happen is what is mistakenly described as dieback. It’s no secret that this is painful. This is MD punishing you to try and prevent you defeating it. The sooner that you can get your head around this the better! This will be your first lesson. Now that you know what is going on, this discomfort should be welcomed not feared.
Then there will be a period of maybe a year where not much appears to be resulting. Don’t be fooled. MD is steadily losing its frontline defence which then disappears as if it were never there. Just stick at it. Close inspection will reveal that the keratinocytes are flowing out of the skin like a liquid metallic glass, which rise up any hair right to the end and then disappears as if it were never there.


The initial response of the normally soft & leathery developmental endospores for the fibres; is to painlessly turn to as hard as stone. Nevertheless, these continue to mature inside and consequently, then ‘ping’ as and when they ‘hatch’, each one of the almost 3 million of these feels like a single nettle sting when they ‘go off’. The keratinocytes have no interest in the spent casings of these, which soften and then rise up and out of the skin; these are dark reddish brown and look like pieces of minute broken eggshells.
Keratinocytes go virtually undetected, even by patients themselves, except for maybe huge deposits under hair on the head which can be felt in the skin against the scalp. Keratinocytes have evolved with a prime directive to lock themselves into the skin and have many strings to their bow to achieve this. A typical sequence of their encouraged demise being;
Around this time, the keratinocytes in the skin will crystallise into a like a continuous sheet of glass which is bonded to every nerve in your skin as if by superglue. One strange happening was that one day I sneezed and broke this ‘glass’ across my stomach, which resulted with feeling like a hernia for a few months. The bad news is; when this separates from the nerves it is a tad painful. The good news is that courtesy off my recommended program I suspect that you will only have to endure this once. I can only suspect this because I endured this every night in cold sweats blipping in and out of consciousness from the pain for more than 9 months before I found the solution.
If I can do that, you can do this and think yourself lucky whilst you’re at it!
I suspect that this pain is the ‘same’ pain as is regularly experienced by sufferers of fibromyalgia? Ironically, that ailment has been correctly identified by medical science as an autoimmune disorder for which they prescribe powerful painkillers. However, medical scientists still have no idea what causes that until they read this.
Now that I have taught doctors what is going on, these medication should/will become available to help you. However, I suspect that this event could be all done and dusted in one unfortunate night to remember?
The microfibres will not appear until after the keratinocytes has/have been mostly released from around it; these then will appear as if by magic. Oxygen is there nemesis. These are the least oxygen tolerant component and which perish before rising out.
These are driven towards the surface literally fizzing and twitching with keratinocytes activity before dying. This fibrous material then clumps together into like little lumps of ‘hat felt’ and can alternatively slowly hydrate into a ‘black glue’ before exfoliating.
Wherever there is keratin (ocytes), the microfibres will be encapsulated inside/below it, which is why the keratinocytes are there. The procedure is; to weaken and dispel the keratinocytes which allows the antibiotics to get at the infection and do their job. Once the antibiotics have gained access to the infection, it still takes several months for this to do its job.
Skin becomes what I can only describe as a bubble-wrap of singularities.
Like billions of empty glass bubbles that burst and flow away like liquid glass.
1 year on full treatment before micro fibres began to rise.
Every single element of MD is designed to by hook or by crook remain anchored in skin.
In response to the Hemp Balm, the keratinocytes that are covertly manifesting in the skin as if it were a sponge inflate just a little into a consistency like sticky putty before then turning into like a continuous sheet of glass that is bonded into the skin as if by superglue. This event is not painful, yet can be uncomfortable especially so when changing sleeping position in bed; which is symptom that you are winning.
I have described the sores as toughened glass and the keratinocytes as standard glass consequent to the way that they behave and feel. Without even looking, it is possible to recognise if the discharge is red or white.
The Hemp Balm neutralises the bio film and the keratinocytes will try to replenish it. This is how the traffic jam begins to move. For the first few months there’s not much evidence to be seen, however, there is no shortage of evidence to be felt. When you get it moving, the keratinocytes float out on the hemp balm looking like liquid glass which migrates up any hair, where it then disappears as if it was never existed!
This ‘sheet of glass’ which forms within the entirety of skin, is fully encompassing and is bonded to the nerves as if by superglue, consequently, as this began to lose adhesion here and there whilst separating; was the most incredibly 10/10 painful time during my remission that went on and on for months. However, at that time I was using the CBD cream that I could only afford to apply once per day, subsequently, I discovered the hemp balm.
I could tattle on, but those are the bones of it. Just stick at it.
Eventually MD will reveal its epicentre of microfibres production to be around and behind the eyes.
This is not painful; however you will look as though you have been in a fight because you have! Next day, there will be no sign that this ever happened. The keratinocytes liquefy and flow out bringing the microfibres along with it.
This will coincide with the time that most sores have gone or are almost gone.
What microfibres remain will be on the scalp, which painlessly steadily lose protection from the keratinocytes and exfoliate. Oxygen is their nemesis. I found Neosporin to be beneficial product at this time. I cannot comment on use of this cream earlier in remission, because I had not tried this until then. Note that bicarbonate of soda is generally the most successful product for nemesis of the sores which are acidophiles. The Neosporin is a more ‘controllable’ product for close proximity around eyes. However, I never once had any eye sting from bathing in it, not even in the dermatologist scaring brew.
Just stick at it until every and all are gone beyond any doubt whatsoever.
Then continue with the program for 3 months to make sure.
When you have beaten MD, please let me know?
Thank you
……………
Tips:
Top Tip: Read the instructions!



When at home don’t wear clothes wear a bath robe, which makes the necessary creaming & rubbing a far simpler task and helps to contain the mess.


Buy hemp balm by the box, it’s cheaper that way and you’re less likely to run out. Don’t throw the pots away without first draining the ‘empties’ that are never empty, into another pot.
Keep a pot of Hemp Balm in the bathroom, another in the bedroom and another next to where you sit. Creaming is less of a task when there’s always a pot handy for the occasions that you’re in a state of undress.
On/over areas when & where keratinocytes are susceptible to hydration the hemp balm will instantly ‘congeal’, when this happens; lay it on here heavily and often.
Stay well stocked with your favourite non alcoholic drinks and have one of these next to you at all times. I suggest that ‘no added sugar’ natural product options could be a more suitable choice. My favourites are/were; sparkling spring water, orange juice & sparkling spring water and unsweetened cranberry juice.
Don’t concern yourself with how long remission may take; exfoliating the smallest amount proves that you can beat MD; this is a marathon not a sprint. Once you appreciate what a challenging task this is, I am confident that you will chose to pursue a steadier pace.
Be content to be getting better, remission is not a race.
Please remember there are more important things in life than remission from MD. You might not think so now, but sooner or later you’ll work this out. Don’t forget to take a day off now and then, simply stop taking THC, keep the hemp balm to a minimum and avoid going out when it’s dark, especially to places that are over 21C and enjoy having a ‘normal’ day or few.
……………
Development of this remedy: I can only test pilot this cure once and there’s a limit to how much that could be discovered on my own.
I tried to share this journey with others, for the benefit of many others, however, these persons who remain uncured, apparently all knew better!
Likewise for the doctors and dermatologists with whom I tried to share this and who continue to cure nobody of MD, because apparently, they all knew better too!
Nevertheless, for those who don’t know better, there is definitely advancement that could be made with improvement for amending skin pH.
Diagnosis: The first symptoms for me were; smells of rotting flesh in my nose and ‘pimples’ around my anus.
How difficult can it be for doctors to see the sores, hairs, fibres and the presence of keratin over cheek bones and to feel the keratin build up in the scalp against the skull, if they had boxes to tick for these, maybe they would cease to be invisible?
Diagnostic Aid 1: Eucerin with 30% Urea, applied to forearms and calves, in around 20 minutes crystallizes and lifts bio film off of the skin into like a remarkably fine sheet of glass that shatters and disappears when touched. (This works only once)
Diagnostic Aid 2: Morgellons disease has its own particular smell, which explains the attraction to flies, I have described this to doctors as like the smell of rotting flesh, the most accurately I can describe this, is like the rotting flesh of a vole.
If I can smell it, dogs could be trained to identify this ailment!
I suspect this aroma is the parasites means of communication?
Early diagnosis would save many woes. For the pimples that formed around my anus immediately after infection, I was prescribed a week’s supply of flucloxacillin and then ignored. This resulted with the back of my neck covered in 15mm round patches that felt like crinkly tissue paper. When I finished the course of antibiotics, these went away.
This proves that this infection is more susceptible to antibiotics if it is caught before it can get dug in.
……………
Conclusions:
Bacteria’s exist in both beneficial and detrimental forms, so it should not be a surprise that archaea do too!
Now that I have revealed this unsurprising fact, I strongly suggest there could/would be further leaps forwards for medical science from capitalising on this revelation!
If microscopes were pointed at remaining mysteries to medical science with the correct focus, more archaea would be found!
I’ll stick my neck out again and suggest that cannabis could be the kiss of death for the entire family of archaea?
Please don’t shoot the messenger before taking a look through the round window!
Exposing MD as an autoimmune disorder exposes that the ‘keratin’ is there, because an archaea infection is there and that ailments with ‘keratosis’ in their titles are autoimmune disorders too. MD could be described as “acute keratosis pilaris”.
H2S exists in varying ‘gravities’ and this strength of concentration I believe dictates how strong this organism can/will become. With MD at the top of this scale and KP at the bottom, other greater and lesser keratosis ailments begin to fit into this jigsaw puzzle.
I surmise that it’s possible for these to be a family of ailments which could manifest from this one organism.
Taking my thoughts a leap of faith further;
With keratinocytes being the immune systems first line of defence and which are shape-shifting multi-capable entities, reveals that other autoimmune disorders could be caused by other archaea organisms with differing influences?
Ironically, the strongest opponents to this cure have been the MD patients themselves!
Some of whom were even inspired to campaign against it!!
This irony I believe to be the underlying root of existence for archaea autoimmune disorders.
Should I be correct, only persons with sufficient strength of character and power of will to overcome this influence will defeat MD, and/or other archaea infections.
Morgellons disease is an autoimmune disorder which I believe is one of a family of autoimmune disorders that each have ‘keratosis’ in their titles and which effect probably more than half of the people on the planet.
I believe that this remedy or a ‘lesser’ variation of could also cure this/these?
This is the first ever cure for any autoimmune disorder and with keratinocytes being both the immune systems first line defence and also the anomaly to resolve, I believe that this remedy or less sledgehammer variations could cure keratosis pilaris and/or skin ailments various that have ‘keratosis’ in their title?
I suspect this/these could even be the same presently ignored infection, which manifests differently resulting from the strength of the ‘infection/organism’?
The pain experienced when keratinocytes are separating from the nerves, I suspect is common with the pain experienced by fibromyalgia sufferers and suspect this remedy or a variation of could also be of benefit for this condition?
I believe there would be benefit from better means of amendment for skin pH.
……………
Sharing:
After more than 400 years of medical mystery, $millions spent on failed research, many $millions paid to doctors who know that they can’t cure this and many $millions more spent on medications that don’t work; you would think that finding a cure would be welcomed with fame, fortune and maybe even a Nobel Prize? However, because I’m not a doctor that is not the case at all, it appears that nobody will take any notice because finding a cure was not my job!
I have tried to help MD patients directly; however, because I did not ask for money, this information was regarded as worthless to them! Ironically and notably, each and every one had excuses to prevent them from getting better, including;
“I won’t take antibiotics!” The most popular reason given; “I have tried those and they didn’t work!”
One of these anti-antibiotics persons picked & mixed from unspecified elements of the program for a week or so; then informed more than 2,000 MD sufferers that this program didn’t work!
“I don’t like baths!”
“I won’t have my hair cut short!”
One woman decided that the best option was to wash her hair in her own urine!
“I don’t like moisturising creams!”
“I won’t cut my beard off!”
“I can’t be bothered to read all that!”
And even;
“Who do you think you are!”
The Moderator of an MD ‘research’ website repeatedly informed more than 2k members not to follow my advice. Notably, he has MD too.
Excuse me, I gave up with this futile exercise; there were more important things to do than flogging dead horses.
The old adage; “You can lead a horse to water but can’t make it drink,” has never been so apt!
……………
Further attempts to share these revelations:
Dermatologists reside in two camps, “There’s nothing wrong with you because there never was.” or “This evidence is worthless without peer reviewed research.” (Which no-one at that time had any interest to perform?)
Subsequently, with support from my local MP, I wrote to the Secretary of State for Health & Social Care, attempting to deliver this information for amendment to doctor’s curriculum and put a stop to the malpractice of administering CBT for a curable skin complaint.
His response however, was to inform me that I was taking the wrong antibiotics!
I have attempted to submit an article to the British Medical Journal; however, this was declined because I am not a doctor!
I have written to a celebrity dermatologist in US. No reply
I have written to Astra Zeneca. No reply
Subsequent to recently spaffing another $600.000 on ‘research’, the CDC reaffirmed that Morgellons Disease is a delusional parasitosis mental health issue and have officially closed the book on it, so I haven’t wasted my time writing to them.
Whilst remission was peaking, I wrote to my GP and requested an appointment for him to officially witness and record this event. No response.
I wrote to the Dispatches Team @ Channel 4. No reply.
I have attempted to upload this dissertation to a site for the attention of a medical scientist who has demonstrated interest in this subject; however, because I’m not a doctor, I’m not allowed to do so. It appears that the ‘system’ has been contrived so that only the blind are permitted to lead the blind!
Saving the best until last, I contacted the Charles E. Holman Morgellons Disease Foundation. However, after writing several emails and sending them a photograph of Salvador and begging for them to review my work, the only thing they were interested in doing was to recommend that I read their failed research, because I have ONLY cured Morgellons Disease once!
“I have unravelled the mystery of Morgellons Disease, revealed its biology, formulated a cure and proven this to work on myself. In between nursing myself, I have written a dissertation explaining all and I’m trying to contact Marianne Middleveen, MDES to ask if she would be willing to peer review this paper?
Thank you”
I’d like to ask you to please read the research studies on Morgellons. I’ll provide quick links below. The journals are mostly open access so you can download the pdf. The science is strong and I think you’ll find it difficult to argue. Also I should add that Dr. Randy Wymore and his team at Oklahoma State University have similar findings although his work is not yet published but will be soon. He and his team have presented at our annual conferences and at Research Day at OSU-CHS in Tulsa, OK.
Also, please go to PubMed and read the publications authored by Anthony Bewley et al. Bewley is no stranger to us as he has long been part of the ‘Opposition” to Morgellons along with his Psychodermatology sub specialty team who mostly have a fixed belief, despite evidence to the contrary, that Morgellons is purely psychiatric in origin. He may prescribe some Doxycycline but this is more of a “rapport enhancing” tactic being used to help convince Morgellons patients to take the anti psychotics such as Pimozide, Resperidol and others.
You can read more about “Rapport enhancing tactics” by searching PubMed for the papers authored by John Koo, MD, FAAD, FAAP, …the king of DOP who is a leading member and perhaps the King of the sub specialty field of Psychodermatology.
We’ve been in this for over 20yrs now and we’ve learned much more than I think you realize.
“I met with Professor Bewley on Tuesday and converted his belief in 5 minutes.
That’s why he has agreed to review my dissertation.
Excuse me, but I’m not going to waste my time reading failed research.
Nobody else has cured this.
I have.”
It seems a bit premature to claim a cure when you’ve only tested your “cure” on one study subject and that is yourself.
We are all volunteers who mostly have Morgellons ourselves. My time can be much better spent with those who are respectful and those who don’t think everybody else is wrong and you are the only one who is right. Especially when you have only one Morgellons study subject!
“Does that mean that you are not interested to learn the cure for Morgellons Disease?
Thank you”
(No reply)
……………
So there you have it; Game, Set & Match!
Maybe ‘Venom’ is not such a distant cousin after all?
MD has such a strong Psychodermatological influence; the MD fraternity officially has no interest in a cure! Despite this cure converting the belief of their ‘opposition’ in minutes, without contradiction, not a single one!
Which must prove beyond any doubt whatsoever that MD has psychological control at a deeper level? Notably: In the exact same frisky manner of taking offence over nothing as my crony who has Fibromyalgia!
So much so, I’m beginning to wonder about the brain fog, this presently undetectable organism can become integrated into the skin, I believe this also becomes integrated into the brain? I’ll leave that one to be pondered over by Professor Bewley and others.
Whatever, MD appears to have met its match with my divergent brain.
Full disclosure about this for the record: I have an eidetic memory and excellent analytical skills which previously have been challenged by Mensa. Every single test resulted with the maximum score of 180 IQ, classification ‘immeasurable’. I have been around the World more times than I can remember and at one time could converse in around a dozen different foreign languages. Fluent in some effluent in others, but certainly good enough to keep me out of trouble and every single one of those was self taught along my way.
With my case, these analytical skills were essential, however, now that a solution has been revealed, you merely need brute determination. I am a very stubborn old man.
This proves that power of will can overcome.
Both Parasitosis and Psychodermatology are real.
………….
My aim is to become cured of MD whilst simultaneously kneading these words into sufficiently understandable format for distribution to as many MD patients as I can reach as soon as I am clear. MD is a slippery subject to grasp, let alone try then to explain; this does however, reveal unexpected connections and it’s not too bad considering this was written in between the creaming and rubbing by an old man with degenerative spine disease, poor eyesight, no microscope and occasional recreational brain fog; whilst ‘normal’ folk and dermatologists were safely tucked up in their beds!
I can’t help but wonder if the recreational brain fog confusticated ‘Venom’?
Whatever, now I have my life back and can resume the pleasant things I have been denied for the last 10 years.
……………
So there you have it, perfect it is not, nevertheless, under the circumstances, way over and above the call of duty it is.
This disease that ‘officially’ doesn’t exist; I have cured not because of medical science yet mostly despite it. By simply using a few of the things that were lurking in my head amongst the fog; in order of application, basic curiosity, basic chemistry, basic physics, basic biology, basic logic, basic psychology, common sense and determination; Only half of which are taught. I have never failed at any challenge in my life; however, the only thing this has achieved is a huge collection of people who hate me and suspect that I actually discovered Psychodermatological archaea infections a very long time ago? I left school at the age of 14 to contribute towards our family income and my knowledge is predominantly self taught, I educated myself in my own time and in my own way with my life mentors being Professor Stanley Unwin and Hieronymus Bosch. This avoided the compulsory bracketing of State education. Consequently, my brain functions properly.
Nevertheless, I now have a fifth hero in my life. Professor Bewley is the only Doctor on the planet that I managed to find who was astute enough to understand what I have been trying to explain to countless doctors for the last 2 years! Thank you very much.
Showing my working out


If the State’s ‘system’ had been sensible enough to work with me instead of against me, they wouldn’t now be licking their wounds, again.
The solution resulted with a remedy that includes a substance that’s not legal in many countries and furthermore, this treatment is classified as ‘holistic’ which dictates that big pharmaceutical companies cannot patent this for profit, consequently, doctors won’t be authorised to prescribe this.
This information is not a secret please share widely.

If there was EVER anything that needed to ‘go viral’; you are looking at it now!
……………
Rosetta Stone:
Joining up a few of the now exposed dots.
With Morgellons Disease now correctly identified as an autoimmune disorder, indicates that other autoimmune disorders that are also mysteries to medical science could also be archaea related too.
I strongly suspect that Keratosis Pilaris could actually be the same organism which did not find H2S of sufficient strength to mature to full MD capability. With this ‘harmless’ organism that affects around half of the people on the planet probably consequently bundled by pathology amongst ‘normal’, possibly the MD infection has subsequently been ignored?
I believe that a ‘lesser’ version of this remedy could cure KP and there’s a list of skin ailments with ‘keratosis’ in their titles which I suspect could be susceptible to common remedy too?
Keratosis Pilaris: I predict to be acidophiles with an anaerobe core.
Bathe not shower, add to the water; 1 pint of bicarbonate of soda, a handful of Epsom salts and a capful of Dettol for luck. Spend an hour soaking in the bath every other day. Allow skin to dry for several hours before then moisturising twice daily, once with a skip over with Neosporin and once, or twice if you like, with a generous slap over of Nivea Hemp Balm. Don’t ask how many times you must do this; just make this your lifestyle and KP will simply fade away.
If this prediction is correct?
That’s around 50% of the World population; 4 billion people cured, right there!
From another archaea acidophile anaerobe autoimmune disorder that was another mystery to medical science.
Fibromyalgia has many common symptoms with MD; brain fog, nerve pain, keratinocytes, sores, lethargy and weight gain and this archaea has the exact same Psychodermatological ‘personality’, which makes me believe that this is the same archaea organism as MD which has matured to become an infectious anaerobic acidophile in a different brew of heavy gasses?
Psychodermatology can identify archaea better than a microscope!
I believe that revealing the MD organism under a microscope will lead to identifying a family of archaea organisms which are each performing a different version of an autoimmune disorder. I suspect that it’s a possibility that many of these could be this same acidophile organism which manifests differently dependent on the recipe and/or weight of heavy gasses that it has matured amongst?
Doxycycline, Neosporin original ointment, bicarbonate of soda, Epsom salts, Corsodyl toothpaste & mouthwash, photoreaction, ambient temperature, O2, hemp products CBD & THC, cod liver oil, hydration, exercise, sunlight a low sugar & fat diet, magnesium and calcium with a shave and a haircut, have all been identified as contributing remedies for a detrimental acidophile anaerobe archaea.
Take the oral products regularly; however, topical products are absolutely definitely better applied with some irregularity. Archaea infections are clever enough to learn how to defend themselves from regular treatment and know how to fight back.
Keep ‘Venom’ guessing and then he’ll be on the wrong foot when you hit him!
Should you have an autoimmune disorder and be tired of your ailment being a mystery to ‘medical science’, if you’re willing to try and help yourself, maybe this program or a bespoke variation of, could be your salvation too?
All that’s required is a bespoke alternative lifestyle.
I believe that MD is the KING of autoimmune disorders and that I received a massive direct hit from the strongest variant, what I have discovered from beheading this King of Kings should I hope now equip medical science to romp through the lesser others like shelling peas?
I will stick my divergent neck out even further to predict that ‘lesser’ variants weigh less.
The H2S involved in my case was as strong/heavy as H2S gets on which MD was floating. Which required an extreme event to have the opportunity to float out of the sewer; however, endospores that mature in less heavy gasses, the infectious fibres produced consequently, weigh less. These lighter heavy gasses are the gasses that are more commonly expelled from sewers, on which these lighter acidophiles can still float, which makes these lesser acidophile anaerobes more common keratosis ailments.
If that wasn’t sticking my neck out far enough; the list of medical mysteries that I claim are archaea that include fibromyalgia and probably all if not most ailments with keratosis in their title and probably others that I haven’t bothered to look at because that’s not why I’m doing this. With MD and fibromyalgia recognised as having psychodermatological influence. It is very hard not to believe that the ‘lesser’ archaea ailment have psychodermatological influence too.
Even if that wasn’t sticking my neck out far enough for you, I have suggested elsewhere that I suspect there is communication between these archaea influenced behaviours, which I suspect is by means of the smell/aroma I have identified. Group behaviour of archaea infected persons maybe could be negatively influenced by this aroma?
With Archaea now identified as responsible for many medical mysteries, which I suspect could manifest as acidophiles and/or alkalophiles. Men in white coats with some litmus paper should I hope now be able to sort out the remaining few autoimmune disorders in their tea break? Using only my mind; it appears that I have resolved more medical mysteries than I can point my stick at, I haven’t even bothered to count these? So I’ll leave a little something for medical science to have a crack at, so that we can find out whether they can carry on counting after they run out of fingers?
Nevertheless, should a few more of these be permitted to point their white coats at cures from nature’s healthcare, rather than maintenance of ailments for petrochemical wealth-care, maybe the final few percent of people on our planet would not have to continue enduring autoimmune disorders that are (were) mysteries to medical science?

I am ABSOLUTELY CERTAIN that the nemesis for this invisible archaea pandemic will be found in the cannabis plant.
Any irritating twats who know fuck all about this yet nevertheless feel inspired to pick & poke at me; can fuck off and leave me well alone until they have evidence that proves me wrong!
I promise these that this imaginary political evidence would be more difficult to find than Schrödinger’s fucking cat”!
……………
Sewage:
The more people there are, the more sewage there is.
Here in the UK, folks are literally swimming in shit, consequent to the water companies stealing the public’s maintenance money to give to their billionaire friends.
I’m neither rocket scientist nor brain surgeon; however, even a child could work this one out?
I can only conclude that public services on both sides of the Atlantic urgently and immediately need to get their SHIT together before ‘Venom’ takes over the World!
……………
Psychodermatology:
I dare not to explain much more than I already have elsewhere in this paper about my personal experiences of psychology, other than; I evicted MD with well practiced and well exercised willpower.
Our ‘modern’ world appears to have forgotten that to allow the mind to think clearly requires silence! Given this opportunity, it’s quite remarkable what this lump of cholesterol can do, even when it’s only firing on 2 cylinders.
It appears that my independent alternative research techniques have exposed the very roots of Psychodermatology and which has proven this abstract field of medical science beyond any doubt.
I will stick my neck out even further and suggest that this parasitic archaea could be capable of developing a symbiotic collaboration of denial between its hosts and which theory will keep Psychodermatology busy for the next 100 years!
I have a crony who has severe Fibromyalgia, who indecently, refuses to even try using hemp balm on her skin! Her ex husband ran a recycling business where there was there was apparently a yard full of festering skips, some of which produced H2S and without doubt other heavy gasses too, which I strongly suspect was the origin of her ailment that without doubt is an archaea too. She is clearly strongly influenced by this abstract. Notably: the merest mention of this possibility instantly results with irrational ‘trouble’ and I get accused of psychosis!!! The exact same as if/when mentioning this possibility to an MD sufferer, who will then instantly ‘rise’ to defend their archaea. In fact she now claims not to remember there being any skips that smelt of H2S because of her extreme brain fog! She’s a retired Civil Servant; this bogus mental health accusations weapon appears to be standard frontline defence by attack practice for public service employees and which makes me wonder how much of this could be archaea related?
Has Venom already taken over the World?
I never had any doubts about the existence of MD or parasitosis and likewise with psychodermatology, even though I have only recently learned of the correct word to use to describe this.
My head is literally overflowing with solutions for medical mysteries that I never knew that I even knew about and which fit together as simple as a jigsaw puzzle. And I wasn’t even looking for these. Should I be interviewed by a sensible doctor whilst this is going on inside my head, I am certain there are more things that I could stump up too.
These things are so abstract that I suspect many or most have never yet been considered; will at least keep the doubters happy with plenty of things for them to pick at. There’s never any shortage of those and I can’t help but wonder if these habitually argumentative deniers might actually have an archaea infection? I have just revealed that half of the people on the planet do have archaea infections, which makes contradiction of this 50/50 and which goes at least half way to proving this theory already?
Achaea infection and negative attitude, I suspect could be horse and carriage?
Excuse me for blurting out these abstracts, at this time I am literally high on happiness, if I could bottle these feelings and sell them, I would be a billionaire in a week and I literally don’t care if these comments could be capitalised on as fuel by bigots. If just one of these turned out to be correct that would be another great leap forwards in medical science, however, I remain confident that these are all sound Psychodermatological theories that I could prove without doubt if I could be bothered. Nevertheless, if my analytical brain can prove to be of further service whilst I’m at it, this is the perfect platform for me to leave these for consideration by other persons who are paid to do so. I did say in for a penny, in for a pound, this list of medical mysteries that has cost $billions for medical science to fail which I have just resolved for free. If that doesn’t earn me the right for my thoughts to be considered other than for ridicule, maybe these irritating folk who have never solved a medical mystery should ask me for a refund?
……………
Doctors: To prevent this dissertation from being consumed by the horror story that it is, I omitted the most HEINOUS of activities that I was forced to endure by ‘doctors’ and the Carolean laws they are governed by. However, should you be fortunate to have a doctor who hasn’t forgotten how to behave like a doctor, please involve them with your remission, they might learn something? Nevertheless, be advised that he/she/it will insist; avoid direct sunlight whilst taking doxycycline, long term antibiotics are bad for the liver, alkaline bathing is bad for the skin, adding Dettol to bathwater is bad for the skin, smoking is bad for your health and cannabis is dangerous
Your options are; take notice of a Nobody who has cured MD, or continue following the advice of around 13,000,000 doctors lead by about 650,000 medical scientists who haven’t?
……………
Excuse me, but such has to be said:
This age old medical mystery was solved & recorded by a severely disabled old man with no medical training and whilst under extreme duress, despite also enduring multiple debilitating diseases and brain fog (Funnel Web Maze Misdirection). Notwithstanding; fighting the ‘world’ on his own, whilst charged and further handicapped by obstructive professional bigots with imaginary false accusations of mental health issues! Which does make you wonder who actually is in need of the CBT?
It was more than 1.5 millennia ago when Hippocrartes established that illness had both physical and rational explanations!
Which begs the question; what has medical science been fucking about at?
I console myself with unique knowledge that sooner or later these ‘doctors’ and ‘medical scientists’ will have to go back to school for compulsory learning of what they have been deliberately ignoring because they have been instructed to do so! Nevertheless, the good news is; at long last these bigots may now be provided with correct boxes to tick for Morgellons Disease?
Should any of my layman’s conclusions or suppositions be subsequently proven off-piste, so be it. In the great scheme of things, such details explained in alternative ‘proper’ medical ways is dotting I’s and crossing T’s. These interpretations resulted with exposing MD’s biology sufficient to find a cure, which achieved my Prime objective.
……………

I have just proven that around 13,000,000 doctors, 650,000 medical scientists and an innumerable amount of bigots were wrong. At 06.30, the last of the last sore exfoliated and it was like the click of a switch; the ‘fog’ is gone; my brain is now firing on all cylinders again and back up to full power.
I AM CURED
MD is dead, long live DP.

GRANDE FINALE
Now that the sores are gone, consequently, the acidophile hive influence has gone and there are no longer keratinocytes with ‘grip’ at the point of exit remaining. The last of the microfibres are flowing out from behind my eyes within ‘liquefied’ keratinocytes. Last night around my eyes inflated as if I had survived 10 rounds against Mike Tyson whilst he was in his prime. Which revealed as I had suspected that this was MD’s microfibres development stronghold; my eyes have now returned to look ‘normal’. There are also billions of fibres that are withdrawing from my skin into the follicles and which are exfoliating like little balls of hat felt, from head to foot. There remains keratin (ocytes) and dead fibres and dead microfibres on/in every part of my body, however, this/these are hydrating with the Hemp Balm and Neosporin is also helping to get this/these on the move too and which are rubbing out without resistance. My skin is now beginning to work properly again. Some areas are very ‘gluey’ and which take a bit of shifting, yet the follicles are not fighting to seal. I’m not sure how long it will take for the last of this debris to clear; there could be another bucketful yet?
The keratin on my back where because of my disabilities I can’t properly get at it, where there is/was fibres yet no microfibres could do with a proper rubbing, but whatever could still be lurking is no longer receiving hive influence and cannot repopulate sores from any possible not quite dead microfibres whilst I am taking antibiotics. The absence of brain ‘fog’ is further evidence to the visual evidence for the absence of acidophile hive influence from sores and I don’t believe there are any fibres producing endospores remaining, they all exfoliated a long time ago, it is now merely diligent housekeeping from here.
It appears that further evidence that I have beaten this is demonstrated by the keratinocytes exfoliation becoming a daytime also activity.
The wonders of archaea will never cease!
Apparently, I am the World authority on this subject, which makes me confident with this prognosis.
Update: (36hrs later) It appears that MD’s last bastion is on my scalp, here there remain a ‘few’ microfibres that are hanging on in/under extremely stubborn keratin, in lines along MD’s route-ways. These however are becoming fewer by the hour and I stand by my prognosis.
The brutal reality is; I am spending too much time pressing buttons and not enough time creaming & rubbing. Nevertheless, I said that I would have this written to coincide with full recovery and whatever I say I will do; I will do. I have never failed at anything that I have been challenged by and this unexpected challenge was no different to any other. I am the most stubborn and determined Old Fart that you could ever meet. To meet this deadline; I have not slept now for at least a week!
Another layman and asked me a simple question about this and my one sentence reply was one of the most amazing revelations that is now added to this document.
My head is full of so much stuff & things about this; I could keep pressing buttons until the cows come home. However, I have now kept my promise to Professor Bewley that I would look into this mystery to medical science. If there remains anything else that he would like to know about this, he simply has to ask!
“Piss I have taken without doubt right the earned I have” in many more mysterious ways than I have revealed. Even so, if you can’t appreciate that, then please don’t go to the same pub as I do. “Taking the piss may this be, deserved well this was”, I am merely telling the fucking truth and bollocks to our political Civil Services fucking correctness, these twisted servants were a greater challenge than resolving the mystery of Morgellons Disease and “lies do not I tell”. I’d sooner be a Yoda than become anointed a fucking Saint!

Professor Anthony Bewley
Nevertheless, I now have a third hero in my life. Professor Bewley is the only Doctor on the planet that I managed to find who was astute enough to understand what I have been trying to explain to countless doctors for the last 2 years! Thank you very much.
I was so impressed; I put him on my Christmas card list; consequently which now totals 4.
I do however, admit that I only told him a ‘little bit’; there is a limit to how much of this reality even a brain such as his can cope with in one hit! Notwithstanding, I was on the meter of a Private Doctor paying for the privilege to educate a Professor!
I now have my life back and I’m itching to go to the pub for pint and chase some women, then to go fishing at the weekend. I am gagging to get back out and smell some roses!
With the USA alone accumulating MD sufferers at around 1 million persons per year, the sooner this information can be peer reviewed by doctors who know less about this than I do and consequently then accepted; the better it will be for many.
Because I’m not a doctor, I was handicapped by the products that were available to me; however, now that medical science has been brow beaten by my revelations, I would hope that these remedial ingredients could soon be bettered?
I am physically and emotionally exhausted.
But that’s not preventing me from feeling like running naked in the street shouting EUREKA!
Or maybe BINGO!?
Nevertheless, there’s no peace for the wicked, I must get my born again brain back into its box and finish writing my homework before collecting any more Green Shield stamps!
I plan to continue with the program for at least another 3 months?
Regaining full brain function is an abstract that I must try to explain. For me, this feels like; stepping into the Stargate, and/or riding a wild horse bareback, and/or being able to soar like an eagle. This is such an amazing experience of freedom that I want to never stop feeling and is far more pleasant than all the other feelings that I have been focussing on for the last 10 years. It’s amazing. I have spent so much time analysing the nasty feelings to work out what made MD tick. I now appear to be hypersensitive to these wonderful normal feelings that I had forgotten about; and I love it.
I hope that others can enjoy this too?
This is overpoweringly emotional, whenever I talk about this I stream with tears of happiness and I don’t give a toss about who may be watching, but that’s not many, about the only people who visit my prison are the postmen.
Nevertheless, I remained alert, because apparently the World was in need a Lert and it was during this infinitesimally smallest moment during that time of my escape that I found Erwin Schrödinger’s cat coughing up a fur ball of MD fibres.

Brain Fog is a Funnel Web Maze in the Brain!
Like I promised at the beginning, I have been on a very deep dive where Angels have feared to tread;
I hope that the BSAC will be proud of me?
It’s amazing what can be found when you understand where and how to look!
……………
Biological Samples: The biological samples that I presented at my last local 6-monthly hospital appointment that was now 25-months ago, were threw straight into the bin, because the dermatologist was offended that these were in sterilised glass jars and not in the plastic pots that he liked!
I have only one biological sample of a Morgellons Disease reproductive endospore.
“Salvador” is presently in solitary confinement in my deep freeze.
This is the first ever archaea reproductive endospore identified.
Medical science doesn’t even know these exist.
I regard this item waaaaaaaaaaaay too valuable to be trusted with a department whose senior member believes that I have a mental health issue.
Professor Bewley has already accepted that Unexplained Dermopathy is the same organism as Morgellons Disease, which 5 minutes previously he would have sworn was a mental health problem. Which I hope appears to be a WTF peer review already in the in the bag, and who again has given me a clean bill of mental health and agreed to review this dissertation. Nevertheless, the previous incorrect diagnosis by the local senior dermatologist continues to influence my GP that I have delusional parasitosis and who both doctors believe that I should be subjected to CBT.
Even a person with psychosis couldn’t make this story up!
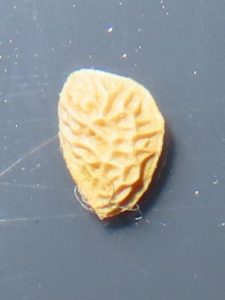
Salvador
This item could/would reveal the final details that debunkers and bigots will “WANT”?
Sealed inside a glass reaction flask and fed with strong H2S whilst being monitored by a macro video camera could/would reveal the final details of this 400 years old medical mystery, once and for all.
I dread to think how long it could/would take to acquire another of these items?
I was hoping that the Charles E. Holman Morgellons Disease Foundation would be ‘keen as mustard’ to get their microscopes pointed at this, their response however, was ‘mean as custard’!
I am certain that this; only one in captivity in the World, unique bullet-proof looking miniature peach stone endospore with an H2S sensing moustache that I have christened Salvador the endospore; is a healthy and viable sample. His inmates also include the secondary fibres endospores that are photographed in this document and more. Most of these will be well preserved dead; however, the fibres in the un-hatched anaerobe endospores may well be protected from oxygen and still ‘alive’? If so, these could be opened in an environment without oxygen and then further ‘proper’ medical science sense could be made of this.
Either way, I believe these also to be of great value to medical science which presently, officially incorrectly claims these to be cotton fibres!
This could/would also confirm or deny my belief that this/these are Archaea.
Should if when there be genuine interest from someone suitably qualified and who is willing to wind their neck in to perform these scientific procedures and save the human race.
Please contact me.
Thank you.
That’ll cost you a fiver to the KO-FI account to help fund this website, I hope that’s not too much to expect?
There is no free email contact address; MD has already fucked up 10 years of my life. Notwithstanding, that would cost me another £6 per month so that folks could then pester me for nothing for the remainder of my life!
……………
I remind you that I’m not a doctor, merely a layman who was motivated to find a cure.
During my conversation about MD with Professor Bewley, his questions I answered with details that I had not explained sufficiently and have since extrapolated on these. Further sensible questions from competent doctors would most probably result with me revealing further details that are presently not included? There are 2 years of my un-proper research stored in my brain. This abstract field of medical science is intrinsically difficult to explain and which inevitably invites addendums. There will always remain further abstract fine details that I could add, however, please excuse me; I also remind you that I am a seriously disabled old man, my spectacles are no longer any use because of this Morgellons shit and consequently, I can barely focus on the screen to see what I’m writing and that using a keyboard traps one of the 6 pinched nerves in my spine resulting with my hands being reduced to spasm and live alone surrounded with lots of things that haven’t been done to make time to explain what was previously unexplainable by herds of highly trained able bodied folk who are generously paid to do so.
I am mentally exhausted from fighting to switch my divergent mind in between the different areas of my brain that is/are/were a maze of funnel webs for me to service the cycle of; recording, collating, editing, analysing and re-recording ad infinitum; that was essential, for my analytical skills to solve this/these list of mystery/mysteries without getting out of my special chair that cossets my degenerating spine. Whilst stuck at home in solitary confinement because most folks have been convinced by medical fucking science that I’m a fucking Nutter. Meanwhile; fielding my wicket from a professional incompetent to keep this idiot off my back serving his own misguided heinous gratification by issuing imaginary Green Shield stamps; to allow me to do the jobs of ‘experts’ for them and I could do with a fucking break!
I wonder if there are any air miles I could claim with my collection of Green Shield stamps?
Been there, done that, have the T shirt and the photographs to prove it.
Now; I would like to put this shit behind me and to move on to whatever may become my next life challenge?
Should I subsequently be distracted from getting on with what remains of my born-again ‘normal’ life; I reserve the right to edit this information for the benefit of improved understanding. Thank you.
I am attempting with great challenge; (That didn’t take very long, did it!) several different alternative avenues to have this dissertation extensively peer reviewed; which does make you wonder, why should I even need to ask? Nevertheless, there will certainly be no shortage of evidence forthcoming for consideration, whichever way the cookies crumble!
This species/family of archaea could be described as malicious parasitic nanobots which take over the control of your whole being.
This parasitic organism is more intelligent than current medical science and which appears to be capable of symbiotic collaboration and which I believe to be a major threat to the human race!
Now is the time that flagellating debunkers will appear from under stones and/or down from ivory towers to rhetorically set fire to their own underpants in public.

I dare you!
There is much to be learned from identifying who these ‘special’ bigots are!
I couldn’t have made this story up, even with the psychosis that I don’t have and suggest to these inevitable persons that they may have an archaea infection?
I have revealed that more than half of the people on our planet already do, which makes this obscure suggestion already more likely than not and statistically substantiates this theory.

I can do no more; if you would like to stop paying for doctors and medications which aren’t curing you, an economic and proven remedy is detailed here for free, the choice is yours…
The worm who turned and saved the human race on his own!
David Payne
20/01/2025

P.S. I was 10 years old when I worked out the origin of the universe, I’m now 69 years old and nobody has taken notice yet; apparently, everyone knows better about that too!
P.P.S.
After medical science eventually admitted there was nothing much it could do to help, it took me a year and a bit to out think this puzzle followed by around 2 years of remission time wasted for millions whilst flogging dead horses to prove it!
I hope those innumerable bigots will be proud of their achievement?
P.P.P.S. I can only Test Pilot this cure once and whilst doing so, also have in each & every which-way done all that I can to be of help to others who are suffering from this complaint, which now includes paying for this site. Should learning how to cure Morgellons Disease have pleased you, buying me a coffee would help to fund this freely given information.
Thank you.

Please let me know when you have your life back and if your gratitude stretches to buying me a beer I can share with your celebration.
……………
Footnote:
This presentation only just got out; during assembly I had a MASSIVE I.T. attack!
I purchased every single premium Avast program and set them onto it?
10 tracking cookies
14 drivers self destructed
Multiple unspecified browser issues
100,772 issues found and the meter is still going like the clappers
The list goes on!
Files were disappearing right before my eyes!
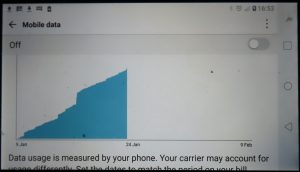
This is where the attack came from and it wasn’t even turned on!
My weight is now down to 80kg, which is somewhere that I haven’t been since I was less than 30 years old.
To meet this deadline; I haven’t had the time to count up; however, I am now beginning to wonder just how many mysteries that I solved for medical science whilst I was asleep?
I think that I’ll just guess at that for now and treat myself to that number of beers?
This most alternative Layman’s Dissertation is to be launched in an hour and the plaque has just fallen off of my teeth!?
The wonders of archaea may never cease?
……………
I will close with my Family Anthem; whilst listening; hear ‘joint’ instead of “bath”.
Supportive Research and Information:
What is Psychodermatology
https://www.britishskinfoundation.org.uk/what-is-psychodermatology-with-dr-anjali-mahto
Addressing the Mind and the Skin Together:
https://www.psychodermatology.co.uk/
Primary Human Keratinocytes:
https://youtube.com/shorts/xnAnQigfxQA?feature=shared
CDC Failed Morgellons Research:
https://stacks.cdc.gov/view/cdc/4362
Scientist Debunks CDC Morgellons “Study”:
https://youtu.be/e37cWrB5-Jk?feature=shared
Medical Science Cloned Blind to MD:
https://youtu.be/BaORnA0e2p0?feature=shared
Marijuana; Super Antibiotic of the Future:
https://realpeoples.media/marijuana-the-super-antibiotic-of-the-future/
Cannabis Compound Helps Fight Resistant Bacteria:
https://www.sciencedaily.com/releases/2020/03/200324131833.htm
How Marijuana Affects the Brain & Body | Dr. Andrew Huberman:
https://www.youtube.com/watch?v=UCbqfBAhmPY
Microbes and the Mind:
https://journals.sagepub.com/doi/abs/10.1177/1745691618809379
Archaea:
Obligate Parasite:
https://en.wikipedia.org/wiki/Obligate_parasite
Many forms of ‘Keratosis’ & Autoimmune Disorders:
Five ways to oxygenate your skin:
Obligate parasitic extremophile organism:
Decoding the roles of extremophilic microbes in the anaerobic environments: Past, Present, and Future:
https://www.sciencedirect.com/science/article/pii/S2666517422000438
Scholarly articles for Obligate Parasitic Extremophile Acidophilic Aerotolerant Anaerobic Thermophilic Archaea:
Photoreactive Crosslinker Chemistry:
Photo-reactive amino acid analogue:
https://en.wikipedia.org/wiki/Photo-reactive_amino_acid_analog
Biological Rhythm:
https://en.wikipedia.org/wiki/Biological_rhythm
Prochlorococcus; Oxygen Producing Bacteria:
Facultative Anaerobic Organism:
https://en.wikipedia.org/wiki/Facultative_anaerobic_organism
Health Benefits of Sea Swimming:
https://www.ancientpurity.com/blog/health-benefits-of-sea-swimming/
Ivor Bigun:
https://youtu.be/YWc1XgmTOfA?feature=shared
……………
Review pending: UK: Professor Bewley, Consultant Dermatologist at Barts Health NHS Trust and Honorary Professor at Queen Mary College (University of London). Special Interest in Psychodermatology.
Review requested: USA: Robert F. Kennedy Jr. The Secretary of Health and Human Services.
(Message for Rupert: If you think that your job is to prevent me from saving the human race?
I point out that there are around 8 billion people who think that you are on the wrong side of a magnetically locked door!)